
» »
Тестостерона ципионат: как и для чего применять в бодибилдинге

Автор: Климишин Юрий — любитель железа и ветеран «химического» фронта.
2015-11-23
Все статьи автора ➤
Важно! Мы не призываем к употреблению стероидов и других сильнодействующих препаратов. Вся информация дана для того, чтобы те, кто всё же решил их принимать, делали это с минимальным риском для здоровья.
Тестостерона ципионат (циклопентилпропионат) — ещё один отдельный (моно) эфир тестостерона, который активно используется в силовых видах спорта. В отличие от энантата и пропионата, у ципионата нет классического периода полураспада. Он лежит в диапазоне от четырёх до восьми дней. Поэтому, не у всех выходит подобрать под себя оптимальную схему использования этого эфира. Но об этом несколько позже. Как и любой другой инъекционный вариант тестостерона, ципионатный эфир обладает всеми положительными качествами присущими этому гормону:
- Хорошая стабилизация андрогенного рецептора;
- Выраженный анаболический и андрогенный эффекты;
- Выдающиеся антикатаболические способности;
- Повышение органической выработки ГР и ИФР – 1;
- Суперкомпенсация гликогена;
- Рост количества специфических рецепторов в мышечной ткани;
- Смазывание суставов (на курсе);
- Усиленная выработка эритроцитов;
- Хорошее воздействие на атлетов с различным опытом использования ААС.
Так же, как и энантат, ципионат легко и просто конвертируется в эстрадиол и дигидротестостерон. Со всеми сопутствующими явлениями. Как положительными, так и отрицательными.
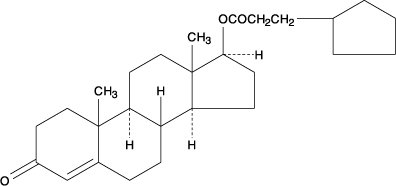
Почему-то принято считать ципионат более дорогой версией тестостерона энантата. Это не так. Если внимательно изучить эфирную цепочку этого эфира, то станет ясно, что наиболее всего она похожа на эфирную цепь фенилпропионата.
Определённые отличия, безусловно, присутствуют, но никакой драматической разницы при этом не наблюдается. Так что, с полным на то основанием, ципионат можно назвать чем-то средним между энантатом и пропионатом.
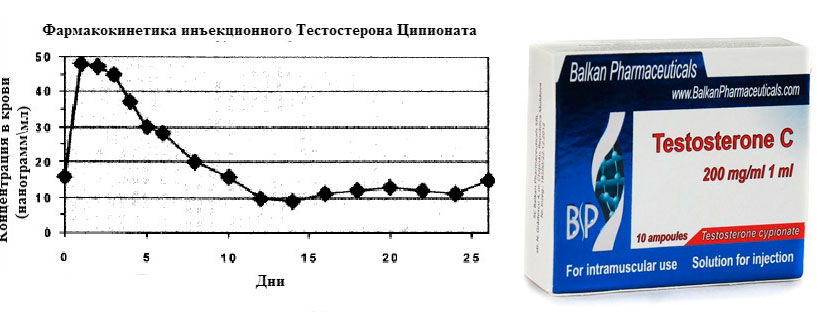
Предельная концентрация тестостерона после укола ципионата наблюдается уже через 48 часов. И может держаться на этом уровне от четырёх до восьми дней. Вот эта неопределённость с периодом полужизни и составляет наибольшую проблему в случае ципионата.
Являясь моно эфиром, он действует ровно и стабильно. Точно так же стабильно его уровень спадает вниз после прекращения активности. Здесь важно, исходя из субъективных ощущений, угадать с периодичностью уколов. Стоит поспешить, и вы столкнётесь с ароматизацией во всей красе. А если опоздаете, то попадёте в гормональную яму и откатите в результатах.
Именно поэтому я и говорил, что не все смогут подружиться с этим эфиром. Но если угадаете, то ципионат станет вашим любимым эфиром тестостерона. Мой совет: начинайте знакомство с тестостероном, пробуя пропионат и энантат. А уже после этого общайтесь с ципионатным эфиром.
Применение
1. НАБОР МАССЫ. Здесь ситуация аналогична энантату. Ципионат поспособствует быстрому и существенному увеличению массы тела (всё те же 10 кг за стандартный десятинедельный курс). Удержать из которых можно порядка половины при грамотном подборе продуктов питания.
Вызовет ощутимую задержку жидкости. В ряде случаев ципионат задерживает воду более интенсивно, чем все остальные инъекционные эфиры тестостерона.
- Повысит общую производительность на тренировках.
- Ускорит восстановление.
- Облегчит процесс повышения силовых показателей.
- Обеспечит накачку мышц кровью и обезболит суставы.
- Защитит мясо от кортизола.
Активная трансформация ципионата в эстрадиол, только во благо массонабору. Вы будете большим, сильным и наполненным на курсе этого андрогена. Кроме того, вас ждут бонусы в виде хорошего настроения, высокого либидо, богатырских сна и аппетита. Это верные спутники любого эфира тестостерона. Действовать и чувствоваться ципионат начинает спустя двое (гораздо реже — трое) суток после укола. Оптимальная продолжительность курса, это 10 – 12 недель.
2. СУШКА. Опять же, если вы угадали с периодичностью инъекций этого эфира, и хорошо чувствуете тестостерон, как таковой, то можно пробовать сохнуть и на ципионате. Но в связи с сильной ароматизацией, длинные моно эфиры мало подходят для периода оформления тушки.
3. ПКТ. Сложный момент. Самым верным выходом будет пойти и сдать анализ на общий тестостерон. Причём, делать это придётся несколько раз (скорее всего). Это в том случае, если у вас не получилось быстро адаптироваться к ципионату. Те, у кого это вышло, сами почувствуют, когда нужно подключать восстанавливающие препараты. В общем, традиционно принято начинать ПКТ спустя два периода полураспада действующего вещества. В случае ципионата, это 8 – 16 дней.
4. Препарат ОДНОЗНАЧНО не для применения женщинами, если они хотят таковыми оставаться.
Дозировки
Объективная недельная доза тестостерона ципионата это 300 – 1000 мг в неделю. Опять же, советую не подниматься выше 500 – 600 мг. Этого более чем достаточно. Периодичность инъекций (пока не научитесь индивидуально подходить к этому моменту) один – два миллилитра каждый третий, четвёртый день. В зависимости от концентрации вещества у отдельного производителя.
Комбинирование с другими ААС
Как и любой другой эфир, тестостерона ципионат может быть единственным гормональным анаболиком на курсе. А может сочетаться с:
- Нандролоном (200 – 400 мг в неделю),
- Тренболоном (200 – 400 мг в неделю),
- Болденоном (600 – 800 мг в неделю),
- Метенолона энантатом (примоболан) (600 – 800 мг в неделю),
- Метандростенолоном (30 – 50 мг в сутки),
- Оксиметолоном (50 – 100 мг в сутки).
На сушке обязательны ингибиторы ароматазы (анастрозол/летрозол) параллельно ципионату. Из стероидов:
- Станозолол (50 – 100 мг в сутки),
- Тренболона ацетат (50 – 100 мг через день),
- Дростанолона пропионат (100 мг через день),
- Местеролон (провирон) (50 – 100 мг в сутки).
При избыточной задержке жидкости на массе (иногда бывает) кушайте ИА (ингибиторы ароматазы) (анастрозол/летрозол). Подробнее о побочных эффектах от тетостерона вы можете прочесть в конце этой статьи.
ПОХОЖИЕ СТАТЬИ
- Тестостерона пропионат – свойства, дозировки и схемы приёма
- Суспензия тестостерона: особенности применения в силовом спорте
- Нюансы сольного использования тестостерона
- Обзор фирм-производителей стероидов
- 10 самых опасных стероидов и прочей «химии»
КОММЕНТАРИИ
Testosterone cypionate is an injectable prescription medication formulated to treat a condition known as ‘hypogonadism’ (where the body doesn’t create enough testosterone). As a compound that can effectively kickstart your testosterone production, it’s little wonder testosterone cypionate has become a huge hit in the bodybuilding community.
Testosterone cypionate is a popular esterified variant of testosterone along with testosterone enanthate (Test E). Let’s look in detail at what exactly testosterone cypionate is, how it differs from testosterone enanthate, how bodybuilders use it and what can be used as a natural alternative if you decide you’d rather avoid using it.
What is testosterone cypionate?
As we touched on above, testosterone cypionate is a prescription medication that bodybuilders tend to self-inject. It’s often prescribed by doctors for men who cannot physically produce enough testosterone, but in recent times, it’s become popular with bodybuilders who believe they may be suffering from low testosterone levels.
Low testosterone hosts a variety of nasty symptoms including weight gain, loss of muscle mass, depression, erectile dysfunction, and gyno-based side effects such as man boobs – none of which are very appealing to a guy hoping to get ripped.
Test C is classified as an androgen; a term used for hormones that fuel male-focused traits such as a deep voice, body hair and of course, muscle mass. Anabolic steroids are another example of an androgenic supplement. Steroids are an androgen-promoting compound; this is why it’s so common for women to develop body hair and a deeper voice when using steroids. On the flip side, the androgenic effects in men result in hair loss (from too much DHT) and organ inflammation.
History of testosterone cypionate
So where did it all start for test cypionate? Well, back in 1951, testosterone cypionate was introduced into the medical community as a prescription drug under the name of ‘Depo-Testosterone’. Kinda catchy, right? Since the 50s, cypionate has been known by several other brand names including ‘Depovirin’, ‘Durandro’, and ‘Duratest’.
Unlike the test cyp of today, the original Depo-Testosterone was used for more than just curing low testosterone production issues. Doctors were also prescribing it for the following:
- Low bone density (weak and fragile bones)
- Osteoporosis
- Muscular atrophy
- Severe menstrual bleeding
As a proven compound for testosterone, you can see how it might become problematic if women and kids start taking it. That’s why, a couple decades later, the FDA restricted the use of cypionate for only cases of hypogonadism and andropause (severely low levels of testosterone).
During the same time another testosterone-focused drug, nearly identical to Test C, made its way into the market – testosterone enanthate. Cypionate is often compared to enanthate (Test E). While both induce higher testosterone levels, the question is often asked: “Is one better than the other?”.
Test E vs test C
A simple internet search will show just how often Test C is compared to Test E. But is there a significant difference between these two testosterone boosters? In short, no. Despite being almost interchangeable as an effective way for bodybuilders to get more testosterone, the debate still rages on bodybuilding forums comparing the miniscule difference between Test C vs Test E.
There’s only one real difference that’s been proven: the chemical makeup. As far as the chemical structure of both compounds goes, in particular, the carbon ester chain, testosterone enanthate is one shy of test cypionate.
Test E has an ester chain, or chemical composition, made up of 7-carbons while Test C has 8-carbons. Does this matter that much? Not really. The only real difference between cypionate and enanthate is that the former is said to break down and assimilate at a slower rate, giving it a longer half-life.
Everything else you hear about the differences between these two is usually found on forums with men and women making different accusations against both Test C and Test E. The most popular examples include bloating caused by cypionate and irritated injection sites caused by enanthate. These examples and several others are more an issue of individual response to a supplement (especially if it’s being abused), than effectiveness.
Testosterone cypionate dosage and cycling

Curious about trying testosterone cyp to increase your t-levels and in turn your gains? You’ll need to have the proper numbers for a safe and effective testosterone cypionate cycle.
The standard testosterone cypionate dosage for beginners is 400 to 500 mg for a 12-week cycle. You’ll be injecting testosterone cypionate three times per week (Monday, Wednesday, and Friday). For those who’ve used testosterone cypionate in the past, the dosage can be increased to 600 or 700 mg; again, this is for a 12-week cycle. The only time you would use less, for example, a testosterone cypionate 200mg dose, would be when you’re stacking it with other anabolic compounds such as Winstrol and Human Growth Hormone (HGH).
Just for your information, the half life of testosterone cypionate is 12 days, compared to 10 or 11 days for testosterone enanthate. So really, not a huge difference at all.
Buying testosterone cypionate injections online
Since testosterone cypionate is an FDA-regulated medication, you’re going to need a prescription to get hold of it legally. If you’re searching for ways to maximize your muscle mass, chances are you don’t really have low testosterone issues, and therefore don’t qualify for that all-important doctor’s prescription. With that said, testosterone cypionate injections are available online.
You can buy testosterone cypionate online from a number of websites; however, many are outsourcing the product from different countries. Without a prescription, the price tag can be incredibly steep and even more worryingly, the products may not be safe, or even genuine. Depending on where you buy testosterone cypionate, the typical testosterone cypionate price for a 200mg vial can range from $50 to $150.
Keep in mind that a dose for a beginner is 400 to 500 mg and you’ll need that amount three times per week for 12 weeks. Best case scenario, you’ll be paying $1,200 for a full cycle. Not cheap by any stretch of the imagination.
A natural alternative to testosterone cypionate
You could spend a ridiculous amount of money on getting hold of testosterone cypionate, and it may not even be the real deal. Even if it is, you run the risk of getting caught with it. And you could enjoy short-lived benefits that need to be backed up by other anabolics, liver therapy or a PCT.
Then again, you could try a natural alternative.
Testo-Max is one such safe, natural alternative. There’s no need for testosterone injections or an insane price tag with this supplement. Its ingredients are scientifically formulated to mimic the effects of testosterone cypionate in a much more gentle, natural way.
Bodybuilders of all ages are skipping test c in favor of Testo-Max. Take a look at it for yourself to see how it could benefit you right here.
Have you tried testosterone cypionate or Testo-Max before? What was your experience? Tell us about it in the comments below.

Be Stronger Than Ever
Supercharge your workouts with some of CrazyBulk’s powerful strength supplements. Enhance your performance and maximize your stamina to unleash the beast inside!
100% legal steroid alternatives – no prescription, no injections, PROVEN RESULTS!
Состав
В состав средства Тестостерона Ципионат входит активный ингредиент тестостерон, который растворен в масляном растворе.
Форма выпуска
Средство выпускается в виде масляного раствора, который применяется для инъекций, содержится в ампулах. Особенности упаковки зависят от производителя препарата.
Фармакологическое действие
Тестостерон Ципионат оказывает выраженное андрогенное и анаболическое влияние на организм человека. При применении средства происходит регуляция функций мужских половых желез, а также процессов синтеза белка в организме.
Тестостерона Ципионат действует относительно медленно, постепенно абсорбируясь в кровоток на протяжении нескольких недель. Как следствие, отмечается нормальный, с точки зрения физиологии, уровень тестостерона в организме, что определяет успешное гормонозаместительное лечение.
Фармакокинетика и фармакодинамика
Тестостерон Ципионат является одноэфирным средством продолжительного действия. Его накопление происходит в основном в жировых тканях организма. После проведения инъекции вещество очень медленно высвобождается. Наибольшая его концентрация в крови наблюдается спустя 24-48 часов после того, как препарат был введен. Как правило, лекарство вводится один раз в неделю.
Маловероятно токсическое влияние на печень.
Показания к применению
Тестостерон Ципионат показан для лечения мужчин при развитии у них следующих заболеваний и состояний:
- половое недоразвитие и нарушения функций половой системы;
- период мужского климакса (после 50-ти летнего возраста) и симптомы, которые проявляются в это время;
- акромегалия (болезнь гипофиза, при которой отмечается увеличение носа, нижней челюсти, стоп, некоторых внутренних органов, а также нарушение обменных процессов в организме);
- гипертрофия простаты.
Женщинам лекарство назначается в следующих случаях:
- период климакса (при условии развития нервных и сосудистых расстройств);
- рак яичников, а также онкологическое заболевание молочной железы (возраст женщины до 60 лет);
- дисфункциональные кровотечения из матки у пожилых женщин.
Противопоказания
Нельзя принимать Тестостерон Ципионат больным раком предстательной железы.
Побочные действия
При приеме больших доз средства у больных может отмечаться состояние выраженного полового возбуждения, задержка солей и воды в организме. Женщины иногда отмечают признаки маскулинизации, то есть появление некоторых мужских черт (сильный рост волос на теле и лице, огрубение голоса), пастозность лица (потеря эластичности кожных покровов лица, небольшие отеки), атрофию молочных желез.
Если женщина принимает слишком больше дозы препарата при дисменореях, вследствие этого у нее может полностью прекратиться менструация.
Также вероятными побочными эффектами является жирность кожи, прыщи, выпадение волос.
Инструкция по применению (Способ и дозировка)
Тестостерон Ципионат необходимо вводить пациентам один раз в две недели, иногда, при некоторых болезнях, инъекции вводят один раз в неделю.
С целью терапии андрогенной недостаточности лекарство вводится по 50-400 мг с интервалом от 2 до 4 недель.
Если препарат используется в спортивных целях, тогда его дозу необходимо увеличить до 200-600 мг в неделю, при этом курсы должны длиться от 6 до 12 недель. В этом случае возможны комбинации препарата с другими средствами.
При лечении женщин дозировку должен определять врач в индивидуальном порядке.
Передозировка
При передозировке ЛС могут проявляться те симптомы, которые являются побочными эффектами при приеме препарата. Необходимо в таком случае приостановить лечение, а продолжить его можно только после полного исчезновения таких признаков. Необходимо уменьшить дозы лекарства.
Взаимодействие
Воздействие препарата снижается, если принимать его одновременно с с индукторами ферментов микросомального окисления.
Условия продажи
В аптеках можно купить ЛС по рецепту.
Условия хранения
Относится к списку Б. Хранить его нужно в темном месте.
Срок годности
Тестостерон Ципионат можно хранить 3 года. Нельзя применять средство после истечения этого срока.
Особые указания
Осторожно средство нужно применять в пожилом возрасте, так как возможно развитие гиперплазии предстательной железы. Желательно регулярно исследовать простату, чтобы исключить развитие онкологических болезней.
Следует с осторожностью назначать препарат людям с отеками, так как под его воздействием в организме может задерживаться натрий и вода.
С осторожностью применяется для терапии подростков.
Аналоги
Совпадения по коду АТХ 4-го уровня:
Аналогичное воздействие на организм пациента оказывают препараты Тестостерон Пропионат, Андрофорт, Вирормон, Аговирин, Андронат, Гомостерон, Малестрон, Пренандрен, Стерандрил, Тестовирон.
Детям
Для лечения детей средство использовать не рекомендуется.
При беременности и лактации
В период беременности, а также кормления грудью Тестостерон Ципионат применять не следует.
Отзывы о Тестостерон Ципионат
Отзывы свидетельствуют, что препарат является достаточно эффективным средством как для пациентов, у которых диагностированы определенные заболевания, так и для спортсменов с целью набора мышечной массы.
Однако отзывы свидетельствуют, что при приеме этого лекарства у многих спортсменов значительно повышается аппетит. При этом отмечается, что набор мышечной массы происходит относительно быстро.
Цена, где купить
Цена Тестостерон Ципионат составляет от 1500 рублей за 5 ампул.
Hormone Replacement in Men
Alicia Stanton MD, in Integrative Medicine (Third Edition), 2012
Dosage
Testosterone cypionate is one of the most widely used intramuscular testosterone esters. At a dose of 200 to 250 mg, the optimal injection interval is 2 to 3 weeks, but peak and trough values are clearly higher and lower than the normal range.129 More often, it is dosed more frequently at 50 to 100 mg once or twice a week, to avoid the high peaks and troughs. In addition, it can be dosed subcutaneously at 30 to 50 mg twice a week. Many of my patients tolerate subcutaneous administration well. It is easy for them to self-administer and does not cause significant peak or trough symptoms.
Read full chapter
URL:
https://www.sciencedirect.com/science/article/pii/B9781437717938000340
Drugs and reproduction
Philip GA Thomas, Alain Fontbonne, in Small Animal Clinical Pharmacology (Second Edition), 2008
Testosterone and derivatives
Widely used in the past for a variety of conditions, testosterone is of no clinical use in small animal reproduction. The 19-nor-steroid mibolerone is the only related drug of use.
EXAMPLES
Testosterone cypionate, testosterone propionate and testosterone ethanate are synthetic esters of testosterone. Mibolerone or dimethyl-nortestosterone is a synthetic, androgenic, anabolic steroid.
Mechanism of action
Mibolerone blocks the release of LH from the anterior pituitary by negative feedback.
Clinical applications
Mibolerone is labeled in the USA for estrus prevention in bitches. Testosterone derivatives have been promoted as stimulants of libido, spermatogenesis and infertility, with no data supporting these claims.
Formulations and dose rates
For estrus postponement, beginning at least 30 d prior to pre-estrus in the bitch but not prior to the first estrus
- •
-
The dose of mibolerone is weight and breed dependent (0.5–12 kg, 30 μg/d; 12–23 kg, 60 μg/d; 23–45 kg, 120 μg/d; >45 kg, 180 μg/d; and German shepherd type-bitch, 180 μg/d PO)
- •
-
Treatment can continue for a maximum of 2 years. However, the drug is not recommended in bitches that will be mated.
- •
-
It has been proposed that mibolerone may be used for the same purpose in cats but this use is not recommended because of the narrow therapeutic index.
Pharmacokinetics
Mibolerone is well absorbed from the gastrointestinal tract, metabolized in the liver and excreted in the urine and feces.
Adverse effects
Mibolerone may induce:
- •
-
premature epiphyseal closure
- •
-
clitoral enlargement and vaginitis, especially in immature bitches
- •
-
abnormal behavior
- •
-
urinary incontinence
- •
-
riding behavior
- •
-
epiphora
- •
-
hepatic changes
- •
-
increased renal weight in adults.
Adverse effects usually resolve after discontinuation of therapy, with the exception of clitoral hypertrophy.
Contraindications and precautions
Mibolerone is contraindicated in:
- •
-
dogs with androgen-dependent conditions
- •
-
pregnancy (it causes masculinization of female fetuses)
- •
-
lactating bitches
- •
-
Bedlington terriers
- •
-
dogs with hepatic or renal disease.
Fatalities have been reported in cats treated with doses as low as 120 μg/d.
Known drug interactions
Mibolerone should not be used concurrently with progestins or estrogens.
Read full chapter
URL:
https://www.sciencedirect.com/science/article/pii/B9780702028588500257
The Transsexual Male
A. Evan Eyler MD, Jamie Feldman MD, PhD, in Clinical Men’s Health, 2008
Simple, “Steady-State” Testosterone Supplementation Programs Are Preferred
Androgen supplementation has traditionally been administered by injection of testosterone cypionate or testosterone enanthate every 1–3 weeks. These treatment programs produce an initial peak in serum testosterone, sometimes at a supraphysiologic level, followed by a gradual diminution over the time preceding the next injection. This pattern is quite different than the usual minor diurnal variations experienced by natal males. Many physicians are now prescribing testosterone patches or gel for their transgendered male patients. These preparations provide less variability in serum testosterone levels, and the patches somewhat mimic the usual diurnal variation of natal males.121 Testosterone 1% gel is easy to use, aesthetic, and generally well accepted by transgendered male patients,122 although some develop skin irritation. In addition, patches and gel can be administered by the patient without the need for training in injection technique.
Read full chapter
URL:
https://www.sciencedirect.com/science/article/pii/B9781416030003100309
Endocrinology
Stan K. Bardal BSc (Pharm), MBA, PhD, … Douglas S. Martin PhD, in Applied Pharmacology, 2011
Androgens
Description
Androgens are male sex hormones.
Common Drugs
- ▪
-
Testosterone
- ▪
-
Testosterone esters: testosterone undecanoate, testosterone cypionate, testosterone enanthate
- ▪
-
17α-alkylated androgens: danazol, methyltestosterone, oxandrolone, stanozolol, fluoxymesterone
MOA (Mechanism of Action)
- ▪
-
Testosterone can be converted in the body to DHT (another physiologically active androgen) and also to estradiol (an estrogen).
- ▪
-
Physiologic androgens will act on androgen receptors to produce the following:
- ▴
-
Male sex organ differentiation in utero
- ▴
-
Secondary sex characteristics during puberty, including libido (sex drive)
- ▴
-
Prostate gland stimulation (growth)
- ▪
-
It is important to note that exogenous androgen administration will result in inhibition of the physiologic sex hormone axis and will significantly inhibit production and secretion of naturally produced sex hormones in both men and women. See Figure 14-10.
Pharmacokinetics
- ▪
-
Androgens administered orally undergo extensive first-pass hepatic metabolism. Therefore modifications to the hormone and also alternative methods of delivery have been developed.
- ▪
-
Androgens can be administered via the oral, transdermal, sublingual, or injection route.
- ▪
-
Testosterone esters are more lipophilic and therefore well absorbed in fat (subcutaneous injections). A depot form of injection (slow release) is the ester testosterone undecanoate.
- ▪
-
17α-Methylated androgens (they have a methyl group attached to the 17 carbon) demonstrate reduced hepatic metabolism but also are less androgenic and are hepatotoxic.
Indications
- ▪
-
Male hypogonadism (reduced testicular secretion of testosterone)
- ▪
-
Low libido states
- ▪
-
Heavy menstrual bleeding
Contraindications
- ▪
-
Prostate cancer: Androgens stimulate the growth of prostate tissue and thus would stimulate growth of prostate cancer. In fact, creating the opposite (hypoandronergic states) are part of prostate cancer therapy.
Side Effects
- ▪
-
Salt and water retention from the mild mineralocorticoid effect (remember that aldosterone is a similar steroid hormone)
- ▪
-
Hepatic toxicity with 17α-methylated androgens only
- ▪
-
Masculinization if used in women: hirsutism, deeper voice, baldness, amenorrhea, breast and uterine atrophy, and infertility
- ▪
-
Consequences of anabolic steroid abuse include the following:
- ▴
-
Central nervous system (CNS): Aggression and depression are associated but may also have been present before steroid abuse; difficult to differentiate
- ▴
-
Cardiovascular system: HTN, accelerated atherosclerosis, sudden death, cardiac hypertrophy, cardiac fibrosis
- ▴
-
Male endocrine: testicular atrophy, decreased sperm counts, increased number of abnormal sperm, infertility
- ▴
-
Hepatic: increased liver enzymes and gallstones
- ▴
-
Musculoskeletal system: premature bone growth plate fusion (shorter stature), tendon ruptures
- ▴
-
Skin: increased acne and baldness
Evidence
Female Libido Management
- ▪
-
A Cochrane meta-analysis in 2007 (35 RCTs, N = 4768 women) showed that the addition of testosterone to HRT effectively increased sexual function. Side effects were acne, hair growth, and lower HDL levels.
Heavy Menstrual Bleeding
- ▪
-
A meta-analysis in 2007 (9 RCTs, N = 353 women) showed weak evidence of the superiority of the use of an androgen over NSAIDs or a progesterone IUD for the treatment of heavy bleeding. However, the side effects were greater with the androgen.
FYI
- ▪
-
How to recognize a steroid abuser when you go to the gym:
- ▴
-
Back acne
- ▴
-
Hypogonadism
- ▴
-
Frequently looks at self in mirror
- ▴
-
Never shares weights
- ▪
-
Hirsutism is a male pattern of hair distribution on a woman (e.g., facial and chest hair).
- ▪
-
Amenorrhea is cessation of the menstrual cycle.
- ▪
-
Infertility in both men and women can persist for months or years after abuse of anabolic steroids, because of prolonged suppression of gonadal hormone production.
- ▪
-
Sterone means a ketone derived from a steroid ring. In addition to testosterone, progesterone and aldosterone are also ketone steroids.
Read full chapter
URL:
https://www.sciencedirect.com/science/article/pii/B9781437703108000142
T
In Drugs for the Geriatric Patient, 2007
testosterone
(tes tos’ ter one)
▪ Brand Name(s): Androderm, AndroGel, Delatestryl, Depandro 100, Depo-Testosterone, FIRST-Testosterone, FIRST-Testosterone MC, Striant, Testim, Testoderm, Testoderm TTS, Testopel, Testro AQ, Testro-L.A.
-
Chemical Class: Androgen
-
DEA Class: Schedule III
▪ Clinical Pharmacology:
-
Mechanism of Action: A primary endogenous androgen that promotes growth and development of male sex organs and maintains secondary sex characteristics in androgen-deficient males. Therapeutic Effect: Helps relieve androgen deficiency.
-
Pharmacokinetics: Well absorbed after IM administration. Protein binding: 98%. Undergoes first-pass metabolism in the liver. Primarily excreted in urine. Unknown if removed by hemodialysis. Half-life: 10–20 min.
▪ Available Forms:
- •
-
Cypionate Injection (Depo-Testosterone): 100 mg/ml, 200 mg/ml.
- •
-
Ethanate Injection (Andro LA 200, Delatestryl, Testro-L.A.): 200 mg/ml.
- •
-
Propionate Injection Solution (Depandro 100): 100 mg/ml.
- •
-
Intramuscular Solution: 50 mg/ml (Testro AQ), 100 mg/ml (Testro AQ).
- •
-
Subcutaneous Pellets (Testopel): 75 mg.
- •
-
Topical Gel: 25 mg/2.5 g (AndroGel), 50 mg/5 g (AndroGel, Testim).
- •
-
Topical Cream (FIRST-Testosterone MC): 2%.
- •
-
Topical Ointment (FIRST-Testosterone): 2%.
- •
-
Transdermal Patch: 2.5 mg/day (Androderm), 4 mg/day (Testoderm), 5 mg/day (Androderm), 6 mg/day (Testoderm).
- •
-
Buccal (Striant): 30 mg.
▪ Indications and Dosages:
-
Male hypogonadism: IM 50–400 mg q2–4wk. Subcutaneous (Pellets) 150–450 mg q3–6mo. Transdermal (Patch [Testoderm]) Start therapy with 6 mg/day patch. Apply patch to scrotal skin. Transdermal (Patch [Testoderm TTS]) Apply TTS patch to arm, back, or upper buttocks Transdermal (Patch [Androderm]) Start therapy with 5 mg/day patch applied at night. Apply patch to abdomen, back, thighs, or upper arms. Transdermal (Gel [AndroGel]) Initial dose of 5 mg delivers 50 mg testosterone and is applied once daily to the abdomen, shoulders, or upper arms. May increase to 7.5 g, then to 10 g, if necessary. Transdermal (Gel [Testim]) Initial dose of 5 g delivers 50 mg testosterone and is applied once a day to the shoulders or upper arms. May increase to 10 g. Buccal System (Striant) 30 mg q12h.
-
Breast carcinoma: IM (testosterone aqueous) 50–100 mg 3 times a week. IM (testosterone cypionate or testosterone ethanate) 200–400 mg q2–4wk. IM (testosterone propionate) 50–100 mg 3 times a week.
▪ Contraindications: Cardiac impairment, hypercalcemia, prostate or breast cancer in males, severe hepatic or renal disease
▪ Side Effects
-
Frequent
-
Gynecomastia, acne
-
Females: Hirsutism, deepening of voice, clitoral enlargement that may not be reversible when drug is discontinued
-
Occasional
-
Edema, nausea, insomnia, oligospermia, priapism, male-pattern baldness, bladder irritability, hypercalcemia (in immobilized patients or those with breast cancer), hypercholesterolemia, inflammation and pain at IM injection site
-
Transdermal: Pruritus, erythema, skin irritation
-
Rare
-
Polycythemia (with high dosage), hypersensitivity
▪ Serious Reactions
- •
-
Peliosis hepatis (presence of blood-filled cysts in parenchyma of liver), hepatic neoplasms, and hepatocellular carcinoma have been associated with prolonged high-dose therapy.
- •
-
Anaphylactic reactions occur rarely.
▪ Patient/Family Education
- •
-
Apply the patch to a clean, dry, hairless area of the skin, avoiding bony prominences
- •
-
Do not take any other medications, including OTC drugs, without first consulting the physician
- •
-
Consume a diet high in calories and protein; food may be better tolerated if he or she eats small, frequent meals
- •
-
Weigh oneself every day and report to the physician weight gain of 5 lb or more per week
- •
-
Notify the physician if acne, nausea, vomiting, or foot swelling occurs
- •
-
The female patient should promptly report deepening of the voice and hoarseness
- •
-
The male patient should report difficulty urinating, frequent erections, and gynecomastia
- •
-
Regular monitoring tests and visits to the physician are important
▪ Monitoring Parameters
- •
-
LFTs, lipids, Hct and Hgb
- •
-
Blood pressure
- •
-
Weight
- •
-
Intake and output
- •
-
Electrolytes
- •
-
Signs of virilization
▪ Geriatric side effects at a glance:
- □
-
CNS
- □
-
Bowel Dysfunction
- □
-
Bladder Dysfunction
- □
-
Falls
▪ U.S. Regulatory Considerations
- □
-
FDA Black Box
- □
-
OBRA regulated in U.S. Long Term Care
Read full chapter
URL:
https://www.sciencedirect.com/science/article/pii/B9781416002086500231
Therapeutic Areas I: Central Nervous System, Pain, Metabolic Syndrome, Urology, Gastrointestinal and Cardiovascular
A.W. Meikle, in Comprehensive Medicinal Chemistry II, 2007
6.22.5.3 Adults
A 5 mg delivery dose of a patch or gel system or 200 mg of either testosterone enanthate or cypionate intramuscularly (IM) every 2 weeks is administered for androgen replacement therapy in males with hypogonadism. If IM testosterone enanthate or cypionate is used, an injection of 100 mg produces a better pattern of testosterone levels, but higher doses at less frequent intervals deviate much more from the physiologic normal testosterone range.3
The efficacy of androgen replacement therapy is best assessed by monitoring the patient’s serum testosterone responses,1,2 because variability in response to testosterone therapy in hypogonadal males in libido, potency, sexual activity, feeling of well-being, motivation, energy level, aggressiveness, stamina, and hematocrit is considerable. Increases in body hair, muscle mass and strength, and bone mass may require months to years of therapy. In sexually immature, eunuchoidal males, androgen replacement therapy may also cause secondary sexual characteristics and long bone growth.
When injectable forms of testosterone are administered, testosterone levels during therapy should be in the mid to normal range 1 week after an injection. Some hypogonadal males treated with testosterone esters experience fluctuations in sexual function, energy level, and mood, which are associated with fluctuations in serum testosterone concentrations between injections.
With patch and gel systems the recommended beginning dose is 5 mg testosterone for adults; smaller doses are recommended for some elderly males. Measurement of serum testosterone concentrations about 12 h after application after daily treatment for 7–14 days will provide information about adequate dosing. Then dosing adjustments can be made. Counseling of patients and their partners before beginning androgen replacement is recommended to help reduce or alleviate adjustment problems of increased sexual interest and performance.
Males with prepubertal hypogonadotropic hypogonadism require the combined treatment with human chorionic gonadotropin (hCG) plus human menopausal gonadotropins to initiate sperm production and fertility. In those with a selective deficiency of GnRH, such as Kallmann’s syndrome, pulsatile GnRH therapy has been shown to stimulate testosterone production and spermatogenesis.
Read full chapter
URL:
https://www.sciencedirect.com/science/article/pii/B008045044X001838
Testicular Disorders
Alvin M. Matsumoto, William J. Bremner, in Williams Textbook of Endocrinology (Thirteenth Edition), 2016
Parenteral Testosterone Esters.
Relatively long-acting parenteral 17β-hydroxyl esters of testosterone, testosterone enanthate and testosterone cypionate, are administered by IM injection. These are effective, safe, and relatively practical and inexpensive preparations that have been used for testosterone replacement in hypogonadal men for decades. Transdermal testosterone gel formulations provide more physiologic testosterone levels and are now used more commonly than testosterone ester injections. However, testosterone esters are preferred over transdermal formulations by some hypogonadal men because they are the least expensive formulation available, require less frequent administration, and usually produce higher average serum testosterone concentrations. Given proper instruction, most hypogonadal men (or a family member) are able to self-administer IM testosterone ester injections. Otherwise, testosterone injections need to be administered in a clinic setting.
Esterification of testosterone at the 17β-hydroxyl group increases its hydrophobicity and solubility within an oil vehicle (sesame oil for testosterone enanthate, cottonseed oil for testosterone cypionate). After IM injection, testosterone esters are released slowly from the oil vehicle within muscle and hydrolyzed rapidly to testosterone, which is released into circulation, resulting in relatively high peak serum testosterone concentrations but an extended duration of release. Testosterone enanthate and testosterone cypionate have similar pharmacokinetic profiles, duration of action, and therapeutic efficacy, so they are considered clinically equivalent.515,516
In adults with hypogonadism, the usual starting dose of testosterone enanthate or cypionate is 150 mg to 200 mg IM injection every 2 weeks. After IM administration of 200 mg of testosterone enanthate, serum testosterone levels usually rise above the normal range for 1 to 3 days and then decline gradually over 2 weeks to the lower end of the normal range, or sometimes to below-normal levels, before the next injection (Fig. 19-29).517 The extreme rise and fall of serum testosterone concentrations may cause fluctuations in energy, mood, and libido that are disturbing to some men. Shortening the dosing interval to every 10 days and reducing the dose to 150 mg (i.e., 150-mg IM injection every 10 days) may alleviate symptoms associated with nadir testosterone levels occurring before the next injection. Alternatively, some patients prefer changing the dose of testosterone enanthate or cypionate to 75 to 100 mg IM every week to reduce swings in testosterone concentrations and associated symptoms. Administration of testosterone enanthate at doses of 300 mg IM every 3 weeks or 400 mg IM every 4 weeks produces extremely wide fluctuations in serum testosterone concentrations with markedly supraphysiologic levels for several days after an injection and levels below normal 3 weeks after an injection (see Fig. 19-29).517
Because CDGP in which puberty eventually occurs spontaneously is clinically indistinguishable from delayed puberty caused by permanent hypogonadotropic hypogonadism (e.g., IHH),141,329,330 testosterone treatment usually is not initiated in boys with prepubertal androgen deficiency until they are about 14 years of age (with a bone age of at least 10.5 years). Testosterone therapy is administered intermittently to allow determination of spontaneous puberty, if it occurs. Occasionally, testosterone therapy is started at a younger age if delayed genital development and growth are causing severe psychological distress in affected boys and their families.
In boys with prepubertal androgen deficiency, treatment is initiated with a very low dose of testosterone enanthate or cypionate (e.g., 50 to 100 mg IM injection monthly or 25 to 50 mg every 2 weeks) to prevent premature closure of long bone epiphyses that would compromise adult height.141,329,330 These low doses of testosterone are sufficient to induce some virilization and long bone growth without interfering with the spontaneous puberty that occurs eventually in boys with CDGP. Testosterone treatment is continued for 3 to 6 months and then stopped for 3 to 6 months to assess whether spontaneous pubertal onset occurs. If there is indication that spontaneous puberty is occurring (e.g., testis size > 8 mL), testosterone therapy is discontinued. If there is no evidence of spontaneous puberty, intermittent testosterone treatment is continued. The dose of testosterone enanthate or cypionate is increased gradually to 50 to 100 mg IM every 2 weeks and then to full adult replacement doses over the next several years to mimic the gradual increase in testosterone concentrations that occurs during puberty.
At present, transdermal testosterone formulations are not approved for use in boys with delayed puberty. However, because they circumvent the need for IM injections, low-dose transdermal testosterone patches and gels would provide very useful alternatives for the treatment of prepubertal androgen deficiency in boys, and they are currently not approved for this indication.
A formulation of testosterone undecanoate in castor oil (Aveed, Endo Pharmaceuticals, Malvern, PA) was approved in 2014 for use in the United States for treatment of male hypogonadism. This formulation is administered by slow IM injection into the gluteus muscle at a dose of 750 mg in 3 mL of castor oil initially, followed by another injection of the same dose 4 weeks later and then every 10 weeks to produce and maintain serum testosterone levels within the normal range in most hypogonadal men.518 Steady state is achieved after the third injection, and mean testosterone levels peak in the high-normal range at 7 days after injection and gradually decline over the next 10 weeks to mean nadir levels just above the normal range. Despite this decline in testosterone levels, fluctuations in or recurrence of symptoms of androgen deficiency have not been reported. Although some men experience discomfort with large-volume injections, they are generally tolerated well and have the advantage of fewer injections than shorter-acting testosterone ester formulations.
A different formulation of testosterone undecanoate in a castor oil vehicle (Nebido; Bayer Schering Pharma AG, Berlin, Germany) has been approved and is used in Europe and other countries for testosterone replacement therapy in hypogonadal men.519 It is administered at a dose of 1000 mg in 4 mL IM, followed by another injection of the same dose 6 weeks later and then every 10 to 14 weeks.
Because of the large volume of drug administered and the need for proper injection technique, self-administration of intramuscular testosterone undecanoate is not possible. Coughing may occur in a small number of men immediately after injection of testosterone undecanoate (this also occurs with shorter-acting testosterone ester injections). Although there is no direct evidence for the cause of coughing, it is conjectured to be related to pulmonary oil microembolism (POME) emanating from the large volume of castor oil vehicle that is injected into the muscle with this formulation. For these reasons, the FDA has required a Risk Evaluation and Mitigation Strategy (REMS) for use of testosterone undecanoate that requires training of personnel and certification of the health care facility to ensure proper injection technique (slow IM injection) and adequate monitoring (for 30 minutes) and treatment capability for potential POME or anaphylaxis following injection.
Read full chapter
URL:
https://www.sciencedirect.com/science/article/pii/B9780323297387000198
Volume II
Bradley D. Anawalt, in Endocrinology: Adult and Pediatric (Seventh Edition), 2016
Estrogen Precursors
Exogenous androgens that can be converted to estrogen through aromatization are a common cause of gynecomastia. Intramuscular testosterone enanthate and cypionate increase estradiol concentrations substantially80 and commonly result in gynecomastia for a few weeks after initiation of intramuscular therapy. This adverse effect is most common in hypogonadal boys during testosterone treatment, and it generally remits spontaneously (without treatment) after a few weeks to months after initiation of a physiologic dosage of intramuscular testosterone. Because transcutaneous formulations of testosterone are associated with smaller peaks in testosterone concentrations, physiologic dosages of these formulations might cause less gynecomastia. Adult athletes abusing anabolic androgenic steroids that are aromatizable and men being treated with high-dosage intramuscular testosterone for hypogonadism or contraception also may experience gynecomastia.80,81 When hCG is given exogenously to men with secondary hypogonadism (due to hypothalamic or pituitary disease), it raises testosterone and estradiol concentrations, but because of its LH-like activity, hCG increases aromatization, resulting in a relatively high estrogen to androgen ratio, and therefore may cause gynecomastia. At physiologic dosages of hCG, the gynecomastia usually remits after several weeks to months.
Read full chapter
URL:
https://www.sciencedirect.com/science/article/pii/B9780323189071001402
Short Stature
Omar Ali, in Nelson Pediatric Symptom-Based Diagnosis, 2018
Sex Steroids
Sex steroid treatments may be administered to adolescents with constitutional delay of growth and development. Males with delayed puberty may be treated with testosterone enanthate or cypionate (50-100 mg/month intramuscularly or subcutaneously for 3-6 months; smaller doses given more frequently may be more physiologic and are preferred by some practitioners) to gradually bring about secondary sexual characteristics and accelerated linear growth. This is often gratifying for males and is usually followed by spontaneous pubertal development. The low dose of testosterone is designed to avoid undue advancement of bone age and loss of growth potential. Oxandrolone is a testosterone derivative with fewer androgenic effects than testosterone, and does not aromatize to estrogen, so theoretically it may be preferable to depo-testosterone injections. Several small studies report beneficial effects of oxandrolone in males with constitutional delay of growth and puberty. The usual dose is 2.5 mg daily for anywhere from 3-12 months. Giving oxandrolone (in addition to GH therapy) to females with Turner syndrome leads to better height outcomes than GH alone, so this is frequently done at around age 8-10 in females who are still well short of a normal height. Females with Turner syndrome who started GH relatively early in life are less likely to require the addition of oxandrolone. The usual dose is 0.03-0.05 mg/kg/day. Side effects at this dose are rare, but signs of virilization should prompt a reduction in dose.
Estrogen—Just as males with constitutional delay are treated with androgens, females with pubertal delay and mild short stature may be treated with a short course of estrogen therapy. However, benign constitutional delay is less likely in females (who are more likely to have an underlying pathologic cause such as Turner syndrome) and such treatment is relatively rare. If it is contemplated, care should be taken to exclude other causes of pubertal delay and to use low doses of estrogens because estrogens promote epiphyseal closure.
Read full chapter
URL:
https://www.sciencedirect.com/science/article/pii/B9780323399562000431
Volume II
Nadine G. Haddad, Erica A. Eugster, in Endocrinology: Adult and Pediatric (Seventh Edition), 2016
Boys
The most commonly employed method of sex-steroid replacement therapy in adolescent hypogonadal boys consists of intramuscular depot preparations of testosterone such as testosterone enanthate or cypionate. The typical starting dose is 50 to 100 mg IM every 4 weeks, which is followed by gradual increases of 25 to 50 mg every 6 to 12 months as indicated by rates of growth, skeletal maturation, and pubertal progression. An adult replacement dose of testosterone consists of 200 to 300 mg IM every 2 to 4 weeks, resulting in elevation of serum testosterone levels to within the normal range. Alternate forms of maintenance testosterone replacement include transdermal testosterone patches and testosterone gels.207 Although experience with these preparations during adolescence is limited,208 ongoing investigation may reveal that they are safe and effective for pubertal induction.
In summary, causes of delayed puberty include both a normal variant and abnormalities at any level of the HPG axis. An increasing number of molecular genetic abnormalities have been linked to specific forms of hypogonadism. Sex-steroid replacement leads to successful pubertal induction and the acquisition of adult secondary sexual development.
Read full chapter
URL:
https://www.sciencedirect.com/science/article/pii/B9780323189071001220

Testosterone Cypionate представляет собой самую длинную из известных на сегодняшний день форм тестостерона. В спортивных целях мужским гормоном пользуются на протяжении длительного времени не только мужчины, но и женщины. Благодаря приему тестостерона, наблюдается значительное увеличение основных физиологических показателей, что неизменно влияет на улучшение получаемых в ходе тренировок результатов.
Тестостерон ципионат наиболее популярен и распространен на территории Америки, где сосредоточено основное производство препарата. Этот стероид выпускают и Балканские компании. Пролонгированное действие тестостерона ципионата обусловлено тем, что стероид «посажен» на эфир, что позволяет ему сохраняться в жировом депо в течение пятнадцати дней.
Активное вещество отщепляется и поступает в кровь постепенно. Подобное «поведение» стероида минимизирует число инъекций, что достаточно удобно. Если рассматривать энантат и ципионат, то эти формы тестостерона вполне могут заменять друг друга, а выпускаются только в виде инъекций.
Содержание
- 1 Какой эффект дает прием Тестостерона ципионата?
- 2 Стероидный профиль Testosterone Cypionate
- 3 Курс приема ципионата
- 4 Возможные побочные эффекты
- 5 Отзывы о Testosterone Cypionate
Какой эффект дает прием Тестостерона ципионата?
Введение этого стероида оказывает следующее положительное воздействие:
- Увеличивается мышечный масса. На фоне приема ципионата возникает повышенная гидратация клеток. Вода составляет весомую долю набираемого атлетом объема. Мускулы приобретают внешне привлекательный и выраженный облик. Накапливание жидкости обуславливает феном отката после завершения курса. На воду приходится до третей части от общей массы прироста.
- Повышаются показатели силы.
- Стимулируется синтез эритроцитов. Возрастание кислородной массы в крови позволяет мышцам функционировать гораздо эффективнее, что положительно отражается на выносливости атлета.
- Обеспечивается сперматогенез и половое поведение.
- Повышается качество фосфорного обмена.
- Возникает положительный азотистый баланс. Количество синтезируемого белка гораздо выше распадающегося.
Стероидный профиль Testosterone Cypionate
Стероид демонстрирует:
- 100% анаболического и андрогенного воздействий от тестостерона;
- значимое подавление цепочки гипоталамус-гипофиз-яички;
- отсутствие токсичного влияния для печени;
- высокий уровень эстрогенной конверсии.
Любая форма тестостерона действует посредством анаболических рецепторов. Ципионат не является исключением. Это позволяет в разы увеличить способность гормона сохранять азот, являющийся основным конструктивным элементом для создания белка в мышцах.
Курс приема ципионата
Оптимальной периодичностью введения инъекции считается один раз в семь дней. Пролонгированное действие ципионата позволяет принимать стероид и реже, но такая схема выполнения уколов не обеспечивает оптимально высокий уровень концентрации гормона. Атлетам, стремящимся набрать мышечную массу, необходимо ориентироваться на ежедневную дозировку в 250-500 миллиграммов.
Соло курсы Testosterone Cypionate позволяют получить высокие результаты. Они отлично подходят начинающим атлетам, которым нет необходимости принимать дополнительные препараты. Необходимо понимать, что увеличение оптимальной нормы инъекции свыше 800 миллиграммов не позволит добиться более выраженного анаболического эффекта, но шансы проявления побочных явлений увеличатся.
Комбинированные курсы во многом идентичны соло. Стероид лучше всего сочетать с Нандролоном. Дозировка обоих препаратов составляет около 200 миллиграммов в неделю. Блокировать эстрогенное воздействие позволяет прием Тамоксифена. Его употребляют со второй недели курса по 10 миллиграммов каждый день и заканчивают использовать через четырнадцать дней после отмены ципионата. Чтобы нормализовать секрецию собственного тестостерона, во время курса принимают Провирон, замещаемый в дальнейшем Тамоксифеном.
Возможные побочные эффекты
Стероид демонстрирует высокий уровень ароматизации. Следовательно, вместе с увеличением мышечной массы повышается и концентрация эстрогена, что является причиной развития такого недуга, как гинекомастия, сопровождаемого уплотнением и припухлостью области вокруг сосков. Чтобы предотвратить риски проявления гино, атлеты принимают блокаторы ароматазы и Нолвадекс или Кломид, являющиеся антиэстрогенами.
Побочные явления от приема ципионата зачастую обусловлены высокой конверсией гормона в активную форму дигидротестостерона, проявляются андрогенным характером. В некоторых случаях у атлета может подниматься артериальное давление, наблюдаться рост волос на различных частях тела и на лице или, наоборот, облысение, угревая сыпь, повышенная секреция сальных желез.
Отзывы о Testosterone Cypionate
Феномен отката после отмены курса ципионата полностью предотвратить нельзя, но набранная мышечная масса, вне зависимости от этого, остается на достаточно качественном уровне. Отзывы говорят о том, что побочные эффекты от препарата, за исключение высокого скопления жидкости, практически никогда не проявляются. Ципионат составляет достойную конкуренцию энантату и очень эффективен.
Большинство профессиональных культуристов комбинируют ципионат с другими препаратами, но такой подход не рекомендован новичкам, поскольку увеличивает возможность побочных эффектов. Лидеров среди производителя этого тестостерона нет, но предпочтение следует отдавать американским и европейским производителям, но именно они зачастую принижают дозировки и завышают стоимость.

Курс тестостерона ципионата (прием, дозировки, нежелательные эффекты)
Тестостерон ципионат считается одним из очень длинных эфиров тестостерона. Его очень часто применяют в комбинированных курсах для набора массы мышц. Период жизни (время действия) препарата в человеческом организме может составлять от 15 до 16 дней. Препарат выпускается в виде масляного раствора, который показан на рисунке с правой стороны.
Тестостерон ципионат от Watson Pharma США
Этот вид эфира достаточно широко распространен в Америке. Поэтому даже не удивляет, что американцы применяют его в собственной практике, более того есть утверждения, что вкусы атлетов связаны не только с доступностью препарата если сравнивать с другими эфирами, но и с его анаболическим эффектом от его приема.
Т.е. если сопоставлять тестостерон ЦИПИОНАТ и ЭНАНТАТ с объективной точки зрения, то можно обнаружить что эти два препарата ВЗАИМОЗАМЕНЯЕМЫЕ. Т.е. ни чем не лучше. Они равны (оба продолжительного действия, на основе масел, вводиться при помощи уколов), кто бы что не говорил. Я встречал на многих форумах срачи по данному поводу, но в действительности, как показала практика РАЗНИЦА между препаратами ЦИПИОНАТ и ЭНАНТАТ = несущественная, поэтому руководствоваться при подборе скорее необходимо доступностью препарата, чем его фармакологическими качествами. Но, по правде сказать, ЦИПИОНАТ хрен найдешь, потому что выполняется тока в Америке, а в странах Европы его создает только – Испания. Ещё изготавливается в Молдове, кстати, как говорит практика и статистика, лучшей маркой считается Тестостерон Ципионат от Balkan Pharmaceuticals (Молдова).
Содержание
- Стероидный профиль тестостерона ципионата
- Эффекты от приема тестостерона ципионата
- Курс тестостерона ципионата
- Комбинированный курс
 (курс, тестостерона, ципионата, приять)")
Стероидный профиль тестостерона ципионата
- Классификация: анаболический стероид андрогенного происхождения
- Способ использования: уколы
- Продолжительность действия препарата – 15-16 дней
- Дозировки препарата: Мужчины 250мг – 500мг.
- Из нежелательных эффектов:
- Угревая болезнь (угри): да
- Задержка воды (есть): высокая
- Ароматизация: высокая (требуется антиэстрогены)
- Гинекомастия
- Рост волос на лице и теле
- Облысение по мужскому типу (от генетики зависит)
- Очень высокое выделение сала кожи
- Снижение своей выработки тестостерона: ДА. Собственно это и провоцирует уменьшение размера яичек, но не нужно беспокоиться после ПКТ их размер восстановиться до начальных размеров).
Эффекты от приема тестостерона ципионата
- Увеличение, как массы мышц, так и силы
- За счёт накопления воды оказывает позитивные влияния на суставы
- Делает лучше регенерация после постоянных тренировок
 (курс, тестостерона, ципионата, приять)")
Существенные приросты массы мышц и силы во время его приема. В прочем, как и прочие эфиры тестостерона. Это происходит благодаря тому что тестостерон ципионат (как и дюбой другой эфир) обладает анаболическим, так и андрогенным эффектом. Благодаря этому быстрые приросты массы мышц связаны с большим скоплением воды, за счёт задержки натрия и эстрогенного действия на организм. Но потому как ципионат совсем нетрудно преобразуется в эстрогены, то около 30% набранной массы будет приходиться на жидкость, которая быстро уйдет после завершения вашего курса.
К тому же ципионат также поможет людям у которых проблемы с суставами, в общем он будет полезным для тех, кто жалуется на боли, хруст в плечах и т.д.
Также этот препарат активизирует восстановление клеток в человеческом организме (содействует быстрому восстановлению) после тяжёлых нагрузок физического плана.
Курс тестостерона ципионата
Даже не взирая на то, что это один из наиболее длинных эфиров тестостерона уколы осуществляются только раз в течении недели, дабы сберечь большую концентрацию. Дозировки 250-500 мг на протяжении недели. Продолжительность курса 8-10 нед. Тестостерон ципионат как говорит практика, даёт положительные результаты при проведении курса “СОЛО”. Также внимание свое обратите на то, что увеличения дозировки (800-1000 мг) не сделает лучше результаты (проверено) потому что набора веса будет за счёт жидкости (воды) а вода уйдет и будет очень сильные потери в веса, в общем, будет только хуже потому что возрастет риск нежелательных эффектов, снова же таки проверено.
 (курс, тестостерона, ципионата, приять)")
Так как эфир совсем нетрудно преобразуется в эстрогены необходимо применить ТАМОКСИФЕН (по 10 мг, в день, начиная со второй недели курса и завершая его прием через 2 недели после завершения курса). А имеет смысл применять ПРОВИРОН (прям на курсе, во время его) а после завершения курса тестостерона ципионата поменять ПРОВИРОН на ТАМОКСИФЕН, дабы начать восстановления секреции своего тестостерона.
Комбинированный курс
Как правило можно сочетать ЦИПИОНАТ и с другими анаболическими стероидами (к примеру, ЦИПИОНАТ + НАНДРОЛОН в дозировке по 200 мг на протяжении недели). Но курс соло и комбинированный мало чем отличается. Смотрите сами.
Ну и как обычно необходимо помнить про:
- Правильную диету для набора массы мышц и силы
- Питание для спортивных занятий для набора массы мышц
Потому что без правильного анаболического питания никакой стероид вам не поможет.