
Состав:
Применение:
Применяется при лечении:
Агранулоцитоз,Аддисонический криз,Аллергия,Анафилаксия,Анемия,Анкилозирующий спондилоартрит,Артрит и Артроз,Аспергиллез и Аспергиллема (неинвазивный аспергиллёз),Астма,Астматический статус,Атопический дерматит,Аутоиммунная гемолитическая анемия,Базедова болезнь,Болезнь крона,Болезнь Поцелуев,Бронхиолит,Буллезная Пузырчатка,Васкулит Сетчатки,Васкулитовый Синдром,Височный артериит,Волчанка,Воспалительное состояние,Врожденная гиперплазия надпочечников,Вторичная Надпочечниковая Недостаточность,Гемолитическая анемия,Гепатит,Гиперкальциемия,Гиперкальциемия Злокачественных Новообразований,Гипоксемия,Гипотиреоз,Гломерулонефрит,Дерматит,Дерматит Герпетиформный,Дерматит,Атопический,Дерматит,Контактный,Дерматомиозит,Заболевание крови,Иммуносупрессия,Инфекционная патология,Инфекционный мононуклеоз,Инфекция,Колит,Колит,Язвенный,Легочный фиброз,Лейкоз,Лимфома,Лихорадка,Менингит,Микоз Грибовидный,Милиарный туберкулез,Неврологические нарушения,Нефротический синдром,Орхит,Отек,Отек легких,Отек мозга,Парциальная Красноклеточная Аплазия,Пемфигоид,Пемфигус Вулгарис,Перитонит,Пневмонит,Пневмония,Пневмоцистная Пневмония,Подагра,Подагрический артрит,Полимиалгия Ревматическая,Полимиозит,Полихондрит,Приступ плохого настроения,Протеинурия,Профессиональная астма,Псориатический артрит,Пузырчатка,Пурпура,Рак мозга,Рак,Множественная Миелома,Рак,Плазмоклеточная Миелома,Рассеянный склероз,Ревматическая лихорадка,Ревматоидный артрит,Респираторный Дистресс-Синдром,Ринит,Саркоидоз,Сенная лихорадка,Сердечный приступ,Синдром Запада,Синдром Стивенса-Джонсона,Системная красная волчанка,Склерит,Смешанная Болезнь Соединительной Ткани,Спондилит,Судороги,Сывороточная болезнь,Травма головы,Трихинеллез,Туберкулез,Туберкулез легких,Туберкулезный менингит,Узелковый Полиартериит,Химиотерапия,Храп,Хроническая Обструктивная Болезнь Легких,Хронический активный гепатит,Шок,Эритема,Ювенильный ревматоидный артрит
Страница осмотрена фармацевтом Милитян Инессой Месроповной Последнее обновление 2022-03-19


Внимание!
Информация на странице предназначена только для медицинских работников!
Информация собрана в открытых источниках и может содержать значимые ошибки!
Будьте внимательны и перепроверяйте всю информацию с этой страницы!
Топ 20 лекарств с такими-же компонентами:
Топ 20 лекарств с таким-же применением:
Предоставленная в разделе Estilsonaинформация составлена на основе данных о другом лекарстве с точно таким же составом как лекарство Estilsona. Будьте
внимательны и обязательно уточняйте информацию по разделу в инструкции к лекарству Estilsona непосредственно из упаковки или у фармацевта в аптеке.
more…
Estilsona
Состав
Предоставленная в разделе Состав Estilsonaинформация составлена на основе данных о другом лекарстве с точно таким же составом как лекарство Estilsona. Будьте
внимательны и обязательно уточняйте информацию по разделу Состав
в инструкции к лекарству Estilsona непосредственно из упаковки или у фармацевта в аптеке.
more…
Prednisolone Acetate
Терапевтические показания
Предоставленная в разделе Терапевтические показания Estilsonaинформация составлена на основе данных о другом лекарстве с точно таким же составом как лекарство Estilsona. Будьте
внимательны и обязательно уточняйте информацию по разделу Терапевтические показания
в инструкции к лекарству Estilsona непосредственно из упаковки или у фармацевта в аптеке.
more…
Таблетки
Порошок для приготовления раствора для инъекций
Аллергические заболевания, контактные дерматиты, надпочечниковая недостаточность, тиреоидит, гипотиреоз, прогрессирующая офтальмопатия, бронхиальная астма, астматический статус, ревматизм, ревматоидный артрит, системные заболевания соединительной ткани, аутоиммунная гемолитическая анемия, апластическая анемия, тромбоцитопения, агранулоцитоз, гемобластозы, лейкемия, инфекционный мононуклеоз, шок.
Шок (анафилактический, посттравматический, постгеморрагический, кардиогенный, вследствие истощения или гипотермии), тяжелые аллергические и анафилактические реакции, токсический отек легких, отек мозга, отторжение трансплантатов, острые тяжелые дерматозы, острые заболевания крови, тяжелые инфекционные заболевания (в сочетании с антибиотиками), острая недостаточность коры надпочечников.
Способ применения и дозы
Предоставленная в разделе Способ применения и дозы Estilsonaинформация составлена на основе данных о другом лекарстве с точно таким же составом как лекарство Estilsona. Будьте
внимательны и обязательно уточняйте информацию по разделу Способ применения и дозы
в инструкции к лекарству Estilsona непосредственно из упаковки или у фармацевта в аптеке.
more…
Капли глазные; Раствор для инъекций; Мазь для наружного применения; Драже; Раствор для внутривенного и внутримышечного введения; Субстанция-порошок; Суспензия для инъекций
Таблетка; Мазь; Раствор для инъекций / инфузий
Таблетки
Порошок для приготовления раствора для инъекций
В/в (струйно, затем капельно) или в/м. Доза Преднизолона и продолжительность лечения устанавливается врачом индивидуально, в зависимости от показаний и тяжести заболевания.
При острой недостаточности надпочечников разовая доза препарата составляет 100–200 мг, суточная 300–400 мг.
При тяжелых аллергических реакциях Преднизолон вводят в суточной дозе 100–200 мг в течение 3–16 дней.
При бронхиальной астме препарат вводят в зависимости от тяжести заболевания и эффективности комплексного лечения от 75 до 675 мг на курс лечения от 3 до 16 дней; в тяжелых случаях доза может быть повышена до 1400 мг на курс лечения и более с постепенным снижением дозы.
При астматическом статусе Преднизолон вводят в дозе 500–1200 мг/сут с последующим снижением до 300 мг/сут и переходом на поддерживающие дозы.
При тиреотоксическом кризе вводят по 100 мг препарата в суточной дозе 200–300 мг; при необходимости суточная доза может быть увеличена до 1000 мг. Длительность введения зависит от терапевтического эффекта, обычно до 6 дней.
При шоке, резистентном к стандартной терапии, Преднизолон в начале терапии обычно вводят струйно, после чего переходят на капельное введение. Если в течение 10–20 мин АД не повышается, повторяют струйное введение препарата. После выведения из шокового состояния продолжают капельное введение до стабилизации АД. Разовая доза составляет 50–150 мг (в тяжелых случаях — до 400 мг). Повторно препарат вводят через 3–4 ч. Суточная доза может составлять 300–1200 мг (с последующим снижением дозы).
При острой печеночно-почечной недостаточности (при острых отравлениях, в послеоперационном и послеродовом периодах), Преднизолон вводят по 25–75 мг/сут; при наличии показаний суточная доза может быть увеличена до 300–1500 мг/сут и выше.
При ревматоидном артрите и системной красной волчанке Преднизолон вводят дополнительно к системному приему препарата в дозе 75–125 мг/сут не более 7–10 дней.
При остром гепатите Преднизолон вводят по 75–100 мг/сут в течение 7–10 дней.
При отравлениях прижигающими жидкостями с ожогами пищеварительного тракта и верхних дыхательных путей Преднизолон назначают в дозе 75–400 мг/сут в течение 3–18 дней.
При невозможности в/в введения Преднизолон вводят в/м в тех же дозах. После купирования острого состояния назначают внутрь Преднизолон в таблетках, с последующим постепенным уменьшением дозы.
При длительном приеме препарата суточную дозу следует снижать постепенно. Длительную терапию нельзя прекращать внезапно!
В/в (струйно, затем капельно) или в/м. Доза Estilsonaа и продолжительность лечения устанавливается врачом индивидуально, в зависимости от показаний и тяжести заболевания.
При острой недостаточности надпочечников разовая доза препарата составляет 100–200 мг, суточная 300–400 мг.
При тяжелых аллергических реакциях Estilsona вводят в суточной дозе 100–200 мг в течение 3–16 дней.
При бронхиальной астме препарат вводят в зависимости от тяжести заболевания и эффективности комплексного лечения от 75 до 675 мг на курс лечения от 3 до 16 дней; в тяжелых случаях доза может быть повышена до 1400 мг на курс лечения и более с постепенным снижением дозы.
При астматическом статусе Estilsona вводят в дозе 500–1200 мг/сут с последующим снижением до 300 мг/сут и переходом на поддерживающие дозы.
При тиреотоксическом кризе вводят по 100 мг препарата в суточной дозе 200–300 мг; при необходимости суточная доза может быть увеличена до 1000 мг. Длительность введения зависит от терапевтического эффекта, обычно до 6 дней.
При шоке, резистентном к стандартной терапии, Estilsona в начале терапии обычно вводят струйно, после чего переходят на капельное введение. Если в течение 10–20 мин АД не повышается, повторяют струйное введение препарата. После выведения из шокового состояния продолжают капельное введение до стабилизации АД. Разовая доза составляет 50–150 мг (в тяжелых случаях — до 400 мг). Повторно препарат вводят через 3–4 ч. Суточная доза может составлять 300–1200 мг (с последующим снижением дозы).
При острой печеночно-почечной недостаточности (при острых отравлениях, в послеоперационном и послеродовом периодах), Estilsona вводят по 25–75 мг/сут; при наличии показаний суточная доза может быть увеличена до 300–1500 мг/сут и выше.
При ревматоидном артрите и системной красной волчанке Estilsona вводят дополнительно к системному приему препарата в дозе 75–125 мг/сут не более 7–10 дней.
При остром гепатите Estilsona вводят по 75–100 мг/сут в течение 7–10 дней.
При отравлениях прижигающими жидкостями с ожогами пищеварительного тракта и верхних дыхательных путей Estilsona назначают в дозе 75–400 мг/сут в течение 3–18 дней.
При невозможности в/в введения Estilsona вводят в/м в тех же дозах. После купирования острого состояния назначают внутрь Estilsona в таблетках, с последующим постепенным уменьшением дозы.
При длительном приеме препарата суточную дозу следует снижать постепенно. Длительную терапию нельзя прекращать внезапно!
Внутрь, по 25–50 мг/сут (в 2–3 приема), затем дозу уменьшают до 10–5–2,5 мг. Максимальная разовая доза — 15 мг, суточная — 100 мг.
В/в медленно, при шоке — 250–500 мг, в исключительных случаях — 500–1000 мг. После купирования острых явлений — оральный прием преднизолона.
Противопоказания
Предоставленная в разделе Противопоказания Estilsonaинформация составлена на основе данных о другом лекарстве с точно таким же составом как лекарство Estilsona. Будьте
внимательны и обязательно уточняйте информацию по разделу Противопоказания
в инструкции к лекарству Estilsona непосредственно из упаковки или у фармацевта в аптеке.
more…
Таблетки
Порошок для приготовления раствора для инъекций
Артериальная гипертензия, болезнь Иценко-Кушинга, психозы, почечная недостаточность, остеопороз, язвенная болезнь желудка и двенадцатиперстной кишки, сахарный диабет, бактериальный эндокардит, сифилис, туберкулез, беременность.
Язвенная болезнь желудка и двенадцатиперстной кишки, остеопороз, острые вирусные инфекции, полиомиелит, системные микозы.
Побочные эффекты
Предоставленная в разделе Побочные эффекты Estilsonaинформация составлена на основе данных о другом лекарстве с точно таким же составом как лекарство Estilsona. Будьте
внимательны и обязательно уточняйте информацию по разделу Побочные эффекты
в инструкции к лекарству Estilsona непосредственно из упаковки или у фармацевта в аптеке.
more…
Таблетки
Порошок для приготовления раствора для инъекций
Возбуждение, бессонница, артериальная гипертензия, отеки, гипокалиемия, алкалоз, аменорея, остеопороз, синдром Иценко-Кушинга, гипергликемия, иммунодефицит.
Миастения, остеопороз, нарушения зрения, депрессии, гипертония, гиперкоагуляция, тромбозы, гипокалиемия, гипергликемия.
Передозировка
Предоставленная в разделе Передозировка Estilsonaинформация составлена на основе данных о другом лекарстве с точно таким же составом как лекарство Estilsona. Будьте
внимательны и обязательно уточняйте информацию по разделу Передозировка
в инструкции к лекарству Estilsona непосредственно из упаковки или у фармацевта в аптеке.
more…
При интравагинальном применении передозировка маловероятна.
Симптомы: потеря сознания, головная боль, головокружение, тремор, судороги, тошнота, рвота, диарея (при случайном приеме препарата внутрь).
Лечение: симптоматическое.
Фармакодинамика
Предоставленная в разделе Фармакодинамика Estilsonaинформация составлена на основе данных о другом лекарстве с точно таким же составом как лекарство Estilsona. Будьте
внимательны и обязательно уточняйте информацию по разделу Фармакодинамика
в инструкции к лекарству Estilsona непосредственно из упаковки или у фармацевта в аптеке.
more…
Эльжина® — комбинированный препарат с антибактериальным, противогрибковым и противовоспалительным действием для местного применения в гинекологии.
Орнидазол — противопротозойное средство с противомикробным действием. Эффективен в отношении Trichomonas vaginalis, Entamoeba histolytica, Giardia lamblia (Giardia intestinalis), а также некоторых анаэробных бактерий, таких как Bacteroides spp. и Clostridium spp., Fusobacterium spp., и анаэробных кокков Peptostreptococcus spp. Механизм действия обусловлен угнетением синтеза и повреждением структуры ДНК возбудителей.
Неомицин — антибиотик широкого спектра действия группы аминогликозидов. Активен в отношении ряда грамположительных и грамотрицательных аэробных микроорганизмов. Устойчивость микроорганизмов к неомицину развивается медленно и в небольшой степени. Практически не всасывается через слизистые оболочки.
Преднизолон — дегидрированный аналог гидрокортизона, оказывает противовоспалительное, противоаллергическое и противозудное действие. Способствует быстрому уменьшению зуда и жжения.
Эконазол сочетает в себе противогрибковое действие в отношении дерматофитов Trichophyton spp., Microsporum spp., Epidermophyton spp., дрожжевых и дрожжеподобных грибов рода Candida с антибактериальным действием по отношению к грамположительным бактериям Staphylococcus spp., Streptococcus spp. Механизм действия заключается в подавлении синтеза эргостерола клеточной мембраны грибов. Действует фунгицидно и бактерицидно.
Фармакокинетика
Предоставленная в разделе Фармакокинетика Estilsonaинформация составлена на основе данных о другом лекарстве с точно таким же составом как лекарство Estilsona. Будьте
внимательны и обязательно уточняйте информацию по разделу Фармакокинетика
в инструкции к лекарству Estilsona непосредственно из упаковки или у фармацевта в аптеке.
more…
При интравагинальном применении системная абсорбция активных компонентов незначительна, препарат практически не всасывается с поверхности слизистой оболочки влагалища.
Фармокологическая группа
Предоставленная в разделе Фармокологическая группа Estilsonaинформация составлена на основе данных о другом лекарстве с точно таким же составом как лекарство Estilsona. Будьте
внимательны и обязательно уточняйте информацию по разделу Фармокологическая группа
в инструкции к лекарству Estilsona непосредственно из упаковки или у фармацевта в аптеке.
more…
- Глюкокортикостероиды
Взаимодействие
Предоставленная в разделе Взаимодействие Estilsonaинформация составлена на основе данных о другом лекарстве с точно таким же составом как лекарство Estilsona. Будьте
внимательны и обязательно уточняйте информацию по разделу Взаимодействие
в инструкции к лекарству Estilsona непосредственно из упаковки или у фармацевта в аптеке.
more…
Лекарственное взаимодействие препарата Эльжина® при интравагинальном применении не изучалось. Несмотря на то что активные компоненты, входящие в состав вагинальных таблеток, абсорбируются незначительно, пациенты, принимающие непрямые антикоагулянты, такие как варфарин и аценокумарол, должны соблюдать осторожность и следить за параметрами свертываемости крови. Рекомендуется информировать врача об одновременном лечении другими ЛС.
Estilsona цена
У нас нет точных данных по стоимости лекарства.
Однако мы предоставим данные по каждому действующему веществу
Средняя стоимость Prednisolone Acetate 1 % за единицу в онлайн аптеках от 3.43$ до 12.75$, за упаковку от 40$ до 115$.
Средняя стоимость Prednisolone Acetate 0.5 % за единицу в онлайн аптеках от 4.69$ до 4.69$, за упаковку от 94$ до 94$.
Источники:
- https://www.drugs.com/search.php?searchterm=estilsona
- https://pubmed.ncbi.nlm.nih.gov/?term=estilsona
Доступно в странах
Найти в стране:
А
Б
В
Г
Д
Е
З
И
Й
К
Л
М
Н
О
П
Р
С
Т
У
Ф
Х
Ч
Ш
Э
Ю
Я

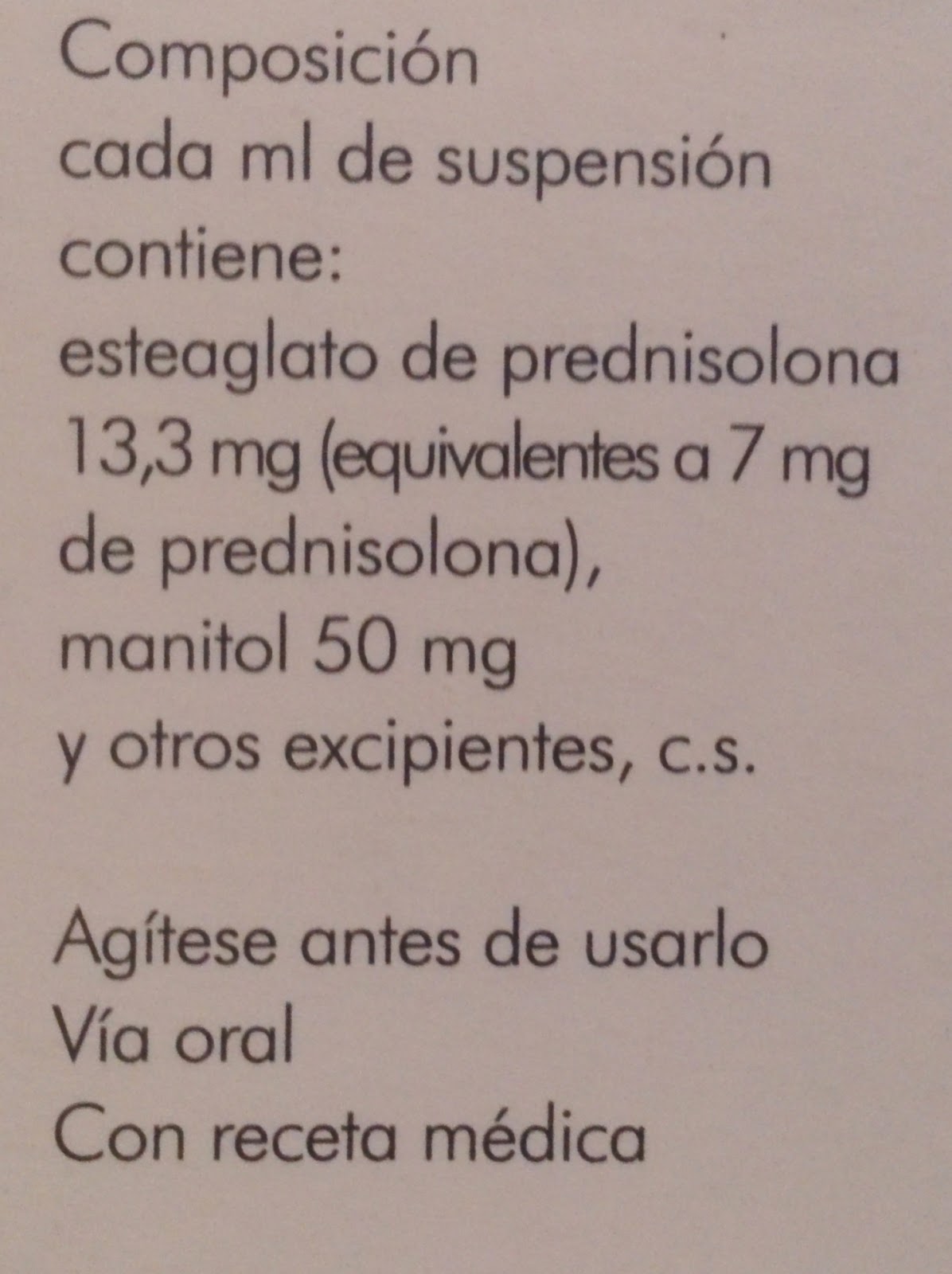
Полная цена 4,29 €, зелёный рецепт — 0,43 €, если ваш годовой доход не превышает 18 тыс. €, и 2,15 — если доход от 18 до 100 тысяч в год.
Широко распространённый в Испании кортикоидный препарат, который применяется как основное лечение при бронхиолите у детей раннего возраста, ларингите, как мощное противовоспалительное и при астматическом статусе.
Дозировка разная, у нас же в райбольнице Испании чаще всего применяют такую:
6 капель х кг веса х в два приёма.
1 мл этой эмульсии содержит 40 капель.
Капельки должны быть только из дозификатора, который прилагается в упаковке флакончика.
Ну а какие там уже дозы выплывают из этого — смотрите на состав именно этой формы лекарственного средства, которое так популярно в нашем госпитале при астматическом статусе.
Не нужно забывать, что средством спасения также является
вентолин, он же сальбутамол
- Antineoplastic Agents
- Glucocorticoids
- Anti-inflammatory Agents
- Adrenergic Agents
- ATC:A07EA01
- ATC:C05AA04
- ATC:D07AA01
- ATC:D07AA03
- ATC:D07AC14
- ATC:D07XA02
- ATC:D10AA02
- ATC:H02AB04
- ATC:H02AB06
- ATC:R01AD02
- ATC:S01BA04
- ATC:S01CB02
- ATC:S02BA03
- ATC:S03BA02
Estilsona
Brand names,
Estilsona
Analogs
- A-Methapred
- Ak-Pred
- Ak-Tate
- Alphadrol
- Articulose-50
- Chloroptic-P S.O.P.
- Co-Hydeltra
- Codelcortone
- Cordrol
- Cortalone
- Cotogesic
- Cotolone
- Decaprednil
- Decortin H
- Delcortol
- Delta F
- Delta-Cortef
- Delta-Stab
- Deltacortenol
- Deltacortril
- Deltacortril Enteric
- Deltahydrocortisone
- Deltasolone
- Deltisilone
- Depo-Medrol
- Derpo Pd
- Dexa-Cortidelt Hostacortin H
- Di-Adreson F
- Dicortol
- Donisolone
- Dydeltrone
- Eazolin D
- Econopred
- Econopred Plus
- Erbacort
- Erbasona
- Estilsona
- Fernisolone
- Fernisolone P
- Fernisolone-P
- Flamasone
- Hostacortin H
- Hydeltra
- Hydeltra-Tba
- Hydeltrasol
- Hydeltrone
- Hydrodeltalone
- Hydrodeltisone
- Hydroretrocortin
- Hydroretrocortine
- I-Pred
- Inflamase Forte
- Inflamase Mild
- Key-Pred
- Klismacort
- Lentosone
- Lite Pred
- M-Predrol
- Medrol
- Medrol Acetate
- Metacortandralone
- Methylprednisolone
- Methylprednisolone Acetate
- Methylprednisolone Sodium Succinate
- Meti-Derm
- Meticortelone
- Meticortelone;Sterolone
- Metreton
- Nisolone
- Nor-Pred T.B.A.
- Ocu-Pred
- Ocu-Pred Forte
- Ophtho-Tate
- Orapred
- PRDL
- Panafcortelone
- Paracortol
- Paracotol
- Pediapred
- Precortalon
- Precortancyl
- Precortilon
- Precortisyl
- Pred Forte
- Pred Mild
- Predair
- Predair A
- Predair Forte
- Predalone 50
- Predalone T.B.A.
- Predate Tba
- Predate-50
- Predcor-25
- Predcor-50
- Predcor-Tba
- Predisolone Sodium Phosphate
- Predne-Dome
- Prednelan
- Predni-Dome
- Prednicen
- Predniliderm
- Predniretard
- Prednis
- Prednisolona [Inn-Spanish]
- Prednisolone Acetate
- Prednisolone Sodium Phosphate
- Prednisolone Tebutate
- Prednisolone [Ban:Inn:Jan]
- Prednisolonum [Inn-Latin]
- Predonin
- Predonine
- Prelone
- Prenolone
- Rolisone
- Scherisolon
- Solone
- Solu-Medrol
- Steran
- Sterane
- Sterolone
- Supercortisol
- Ulacort
- Ultra Pred
- Ultracorten H
- Ultracortene H
- Ultracortene-H
- Ultracortene-Hydrogen
Estilsona
Brand Names Mixture
- Ak Cide Oph Soln (Prednisolone Acetate + Sulfacetamide Sodium)
- Blephamide Oph Ont (Prednisolone Acetate + Sulfacetamide Sodium)
- Blephamide Opht Suspension (Prednisolone Acetate + Sulfacetamide Sodium)
- Canaural (Ear Drops) (Diethanolamine Fusidate + Framycetin Sulfate + Nystatin + Prednisolone)
- Chlorasone (Chloramphenicol + Prednisolone Acetate)
- Delta-Albaplex Tablets (Novobiocin (Novobiocin Sodium) + Prednisolone + Tetracycline Hydrochloride)
- Dioptimyd Ointment (Prednisolone Acetate + Sulfacetamide Sodium)
- Dioptimyd Suspension (Prednisolone Acetate + Sulfacetamide Sodium)
- Liquichlor (Chloramphenicol + Prednisolone + Squalane + Tetracaine)
- Metimyd Oph Sus (Prednisolone Acetate + Sulfacetamide Sodium)
- Optisone (Neomycin + Prednisolone)
- Pred C Tab (Aluminum Hydroxide + Prednisolone + Salicylamide + Vitamin C)
- Prednisize Solution (Camphor + Chlorophenol + Cresyl Acetate + Prednisolone)
- Quiex-Pred Sus (Aminophylline + Guaifenesin + Prednisolone)
- Surolan Drops (Miconazole Nitrate + Polymyxin B Sulfate + Prednisolone Acetate)
- Vanectyl-P Tablets (Prednisolone + Trimeprazine Tartrate)
- Vasocidin Ophthalmic Solution (Prednisolone Sodium Phosphate + Sulfacetamide Sodium)
Estilsona
Chemical_Formula
C21H28O5
Estilsona
RX_link
http://www.rxlist.com/cgi/generic/prednisolone.htm
Estilsona
fda sheet
Estilsona
msds (material safety sheet)
Estilsona
Synthesis Reference
No information avaliable
Estilsona
Molecular Weight
360.444 g/mol
Estilsona
Melting Point
235 oC
Estilsona
H2O Solubility
223 mg/L
Estilsona
State
Solid
Estilsona
LogP
1.705
Estilsona
Dosage Forms
Solution
Estilsona
Indication
For the treatment of primary or secondary adrenocortical insufficiency, such as congenital adrenal hyperplasia, thyroiditis. Also used to treat psoriatic arthritis, rheumatoid arthritis, ankylosing spondylitis, bursitis, acute gouty arthritis and epicondylitis. Also indicated for treatment of systemic lupus erythematosus, pemphigus and acute rhematic carditis. Can be used in the treatment of leukemias, lymphomas, thrombocytopenia purpura and autoimmune hemolytic anemia. Can be used to treat celiac disease, insulin resistance, ulcerative colitis and liver disorders.
Estilsona
Pharmacology
Prednisolone is a synthetic glucocorticoid used as antiinflammatory or immunosuppressive agent. Prednisolone is indicated in the treatment of various conditions, including congenital adrenal hyperplasia, psoriatic arthritis, systemic lupus erythematosus, bullous dermatitis herpetiformis, seasonal or perennial allergic rhinitis, allergic corneal marginal ulcers, symptomatic sarcoidosis, idiopathic thrombocytopenic purpura in adults, leukemias and lymphomas in adults, and ulcerative colitis. Glucocorticoids are adrenocortical steroids and cause profound and varied metabolic effects. In addition, they modify the body’s immune responses to diverse stimuli.
Estilsona
Absorption
Readily absorbed by gastrointestinal tract, peak plasma concentration is reached 1-2 hours after administration.
Estilsona
side effects and Toxicity
LD50=500 mg/kg (oral, rat), short-term side effects include high blood glucose levels and fluid retention. Long term side effects include Cushing’s syndrome, weight gain, osteoporosis, glaucoma, type II diabetes and adrenal suppression.
Estilsona
Patient Information
Patients who are on immunosuppressant doses of corticosteroids should be warned to avoid exposure to chickenpox or
measles. Patients should also be advised that if they are exposed, medical advice should be sought without
delay.
Estilsona
Organisms Affected
Humans and other mammals
<‘Undesirable effects’).
Raised intracranial pressure Raised intracranial pressure with papilloedema (pseudotumour cerebri) associated with corticosteroid treatment has been reported in both children and adults.’Undesirable effects’).
Visual disturbance
Visual disturbance may be reported with systemic and topical corticosteroid use. If a patient presents with symptoms such as blurred vision or other visual disturbances, the patient should be considered for referral to an ophthalmologist for evaluation of possible causes which may include cataract, glaucoma or rare diseases such as central serous chorioretinopathy (CSCR) which have been reported after use of systemic and topical corticosteroids.
Use in the elderly
Treatment of elderly patients, particularly if long term, should be undertaken with caution bearing in mind the more serious consequences of the common side-effects of corticosteroids in old age, especially osteoporosis, diabetes, hypertension, hypokalaemia, susceptibility to infection and thinning of the skin. Close clinical supervision is required to avoid life threatening reactions.
Paediatric population
Corticosteroids cause growth retardation in infancy, childhood and adolescence, which may be irreversible, and therefore long-term administration of pharmacological doses should be avoided. If prolonged therapy is necessary, treatment should be limited to the minimum suppression of the hypothalamo-pituitary adrenal axis and growth retardation. The growth and development of infants and children should be closely monitored. Treatment should be administered where possible as a single dose on alternate days.
WARNINGS
Included as part of the PRECAUTIONS section.
PRECAUTIONS
Alterations in Endocrine Function
Hypothalamic-pituitary-adrenal (HPA) axis suppression, Cushing’s syndrome, and hyperglycemia. Monitor patients for these conditions with chronic use.
Corticosteroids can produce reversible hypothalamic-pituitary adrenal (HPA) axis suppression with the potential for corticosteroid insufficiency after withdrawal of treatment. Drug-induced secondary adrenocortical insufficiency may be minimized by gradual reduction of dosage. This type of relative insufficiency may persist for months after discontinuation of therapy; therefore, in any situation of stress occurring during that period, hormone therapy should be reinstituted. If the patient is receiving corticosteroids already, dosage may have to be increased.
Since mineralocorticoid secretion may be impaired, salt and/or a mineralocorticoid should be administered concurrently. Mineralocorticoid supplementation is of particular importance in infancy.
Metabolic clearance of corticosteroids is decreased in hypothyroid patients and increased in hyperthyroid patients. Changes in thyroid status of the patient may necessitate adjustment in dosage.
Increased Risks Related to Infection
Corticosteroids may increase the risks related to infections with any pathogen, including viral, bacterial, fungal, protozoan, or helminthic infections. The degree to which the dose, route and duration of corticosteroid administration correlates with the specific risks of infection is not well characterized, however, with increasing doses of corticosteroids, the rate of occurrence of infectious complications increases.
Corticosteroids may mask some signs of infection and may reduce resistance to new infections.
Corticosteroids may exacerbate infections and increase risk of disseminated infections.
The use of prednisone in active tuberculosis should be restricted to those cases of fulminating or disseminated tuberculosis in which the corticosteroid is used for management of the disease in conjunction with an appropriate anti-tuberculous regimen.
Chickenpox and measles can have a more serious or even fatal course in non-immune children or adults on corticosteroids. In children or adults who have not had these diseases, particular care should be taken to avoid exposure. If a patient is exposed to chickenpox, prophylaxis with varicella zoster immune globulin (VZIG) may be indicated. If patient is exposed to measles, prophylaxis with pooled intramuscular immunoglobulin (IG) may be indicated. If chickenpox develops, treatment with antiviral agents may be considered.
Corticosteroids should be used with great care in patients with known or suspected Strongyloides (threadworm) infestation. In such patients, corticosteroid-induced immunosuppression may lead to Strongyloides hyperinfection and dissemination with widespread larval migration, often accompanied by severe enterocolitis and potentially fatal gram-negative septicemia.
Corticosteroids may exacerbate systemic fungal infections and therefore should not be used in the presence of such infections unless they are needed to control drug reactions.
Corticosteroids may increase risk of reactivation or exacerbation of latent infection.
If corticosteroids are indicated in patients with latent tuberculosis or tuberculin reactivity, close observation is necessary as reactivation of the disease may occur. During prolonged corticosteroid therapy, these patients should receive chemoprophylaxis.
Corticosteroids may activate latent amebiasis. Therefore, it is recommended that latent amebiasis or active amebiasis be ruled out before initiating corticosteroid therapy in any patient who has spent time in the tropics or any patient with unexplained diarrhea.
Corticosteroids should not be used in cerebral malaria.
Alterations in Cardiovascular/Renal Function
Corticosteroids can cause elevation of blood pressure, salt, and water retention, and increased excretion of potassium and calcium. These effects are less likely to occur with the synthetic derivatives except when used in large doses. Dietary salt restriction and potassium supplementation may be necessary. These agents should be used with caution in patients with congestive heart failure, hypertension, or renal insufficiency.
Literature reports suggest an apparent association between use of corticosteroids and left ventricular free wall rupture after a recent myocardial infarction; therefore, therapy with corticosteroids should be used with great caution in these patients.
Use in Patients with Gastrointestinal Disorders
There is an increased risk of gastrointestinal perforation in patients with certain GI disorders. Signs of GI perforation, such as peritoneal irritation may be masked in patients receiving corticosteroids.
Corticosteroids should be used with caution if there is a probability of impending perforation, abscess, or other pyogenic infections; diverticulitis; fresh intestinal anastomoses; and active or latent peptic ulcer.
Behavioral and Mood Disturbances
Corticosteroids use may be associated with central nervous system effects ranging from euphoria, insomnia, mood swings, personality changes, and severe depression, to frank psychotic manifestations. Also, existing emotional instability or psychotic tendencies may be aggravated by corticosteroids.
Decrease in Bone Density
Corticosteroids decrease bone formation and increase bone resorption both through their effect on calcium regulation (i.e., decreasing absorption and increasing excretion) and inhibition of osteoblast function. This, together with a decrease in the protein matrix of the bone secondary to an increase in protein catabolism, and reduced sex hormone production, may lead to inhibition of bone growth in children and adolescents and the development of osteoporosis at any age. Special consideration should be given to patients at increased risk of osteoporosis (i.e., postmenopausal women) before initiating corticosteroid therapy and bone density should be monitored in patients on long term corticosteroid therapy.
Ophthalmic Effects
Prolonged use of corticosteroids may produce posterior subcapsular cataracts, glaucoma with possible damage to the optic nerves, and may enhance the establishment of secondary ocular infections due to fungi or viruses.
The use of oral corticosteroids is not recommended in the treatment of optic neuritis and may lead to an increase in the risk of new episodes.
Intraocular pressure may become elevated in some individuals. If corticosteroid therapy is continued for more than 6 weeks, intraocular pressure should be monitored.
Corticosteroids should be used cautiously in patients with ocular herpes simplex because of possible corneal perforation. Corticosteroids should not be used in active ocular herpes simplex.
Vaccination
Administration of live or live, attenuated vaccines is contraindicated in patients receiving immunosuppressive doses of corticosteroids. Killed or inactivated vaccines may be administered; however, the response to such vaccines cannot be predicted. Immunization procedures may be undertaken in patients who are receiving corticosteroids as replacement therapy, e.g., for Addison’s disease.
While on corticosteroid therapy, patients should not be vaccinated against smallpox. Other immunization procedures should not be undertaken in patients who are on corticosteroids, especially on high dose, because of possible hazards of neurological complications and a lack of antibody response.
Effect on Growth and Development
Long-term use of corticosteroids can have negative effects on growth and development in children.
Growth and development of pediatric patients on prolonged corticosteroid therapy should be carefully monitored.
Use in Pregnancy
Prednisone can cause fetal harm when administered to a pregnant woman. Human and animal studies suggest that use of corticosteroids during the first trimester of pregnancy is associated with an increased risk of orofacial clefts, intrauterine growth restriction, and decreased birth weight. If this drug is used during pregnancy, or if the patient becomes pregnant while using this drug, the patient should be apprised of the potential hazard to the fetus.
Neuromuscular Effects
Although controlled clinical trials have shown corticosteroids to be effective in speeding the resolution of acute exacerbations of multiple sclerosis, they do not show that they affect the ultimate outcome or natural history of the disease. The studies do show that relatively high doses of corticosteroids are necessary to demonstrate a significant effect.
An acute myopathy has been observed with the use of high doses of corticosteroids, most often occurring in patients with disorders of neuromuscular transmission (e.g., myasthenia gravis), or in patients receiving concomitant therapy with neuromuscular blocking drugs (e.g., pancuronium). This acute myopathy is generalized, may involve ocular and respiratory muscles, and may result in quadriparesis. Elevation of creatine kinase may occur. Clinical improvement or recovery after stopping corticosteroids may require weeks to years.
Kaposi’s Sarcoma
Kaposi’s sarcoma has been reported to occur in patients receiving corticosteroid therapy, most often for chronic conditions. Discontinuation of corticosteroids may result in clinical improvement.
Nonclinical Toxicology
Carcinogenesis, Mutagenesis, Impairment of Fertility
Prednisone was not formally evaluated in carcinogenicity studies. Review of the published literature identified carcinogenicity studies of prednisolone, the active metabolite of prednisone, at doses which were less than the typical clinical doses. In a 2-year study, male Sprague-Dawley rats administered prednisolone in drinking water at a dose of 368 mcg/kg/day (equivalent to 3.5 mg/day in a 60-kg individual based on a mg/m² body surface area comparison) developed increased incidences of hepatic adenomas. Lower doses were not studied, and therefore, a no effect level could not be identified. In an 18-month study, intermittent oral gavage administration of prednisolone did not induce tumors in female Sprague-Dawley rats when given 1, 2, 4.5, or 9 times per month at 3 mg/kg prednisone (equivalent to 29 mg in a 60-kg individual based on a mg/m² body surface area comparison).
Prednisone was not formally evaluated for genotoxicity. However, in published studies prednisolone was not mutagenic with or without metabolic activation in the Ames bacterial reverse mutation assay using Salmonella typhimurium and Escherichia coli, or in a mammalian cell gene mutation assay using mouse lymphoma L5178Y cells, according to current evaluation standards. In a published chromosomal aberration study in Chinese Hamster Lung (CHL) cells, a slight increase was seen in the incidence of structural chromosomal aberrations with metabolic activation at the highest concentration tested, however, the effect appears to be equivocal. Prednisolone was not genotoxic in an in vivo micronucleaus assay in the mouse, though the study design did not meet current criteria.
Prednisone was not formally evaluated in fertility studies. However, menstrual irregularities have been described with clinical use.
Use In Specific Populations
Pregnancy
Teratogenic Effects
Pregnancy Category D : Multiple cohort and case controlled studies in humans suggest that maternal corticosteroid use during the first trimester increases the rate of cleft lip with or without cleft palate from about 1/1000 infants to 3-5/1000 infants. Two prospective case control studies showed decreased birth weight in infants exposed to maternal corticosteroids in utero.
RAYOS was not formally evaluated for effects on reproduction. Published literature indicates prednisolone, the active metabolite of prednisone, has been shown to be teratogenic in rats, rabbits, hamsters, and mice with increased incidence of cleft palate in offspring. In teratogenicity studies, cleft palate along with elevation of fetal lethality (or increase in resorptions) and reductions in fetal body weight were seen in rats at maternal doses of 30 mg/kg (equivalent to 290 mg in a 60 kg individual based on mg/m² body surface comparison) and higher. Cleft palate was observed in mice at a maternal dose of 20 mg/kg (equivalent to 100 mg in a 60 kg individual based on mg/m² comparison). Additionally, constriction of the ductus arteriosus has been observed in fetuses of pregnant rats exposed to prednisolone.
In humans, the risk of decreased birth weight appears to be dose related and may be minimized by administering lower corticosteroid doses. It is likely that underlying maternal conditions contribute to intrauterine growth restriction and decreased birth weight, but it is unclear to what extent these maternal conditions contribute to the increased risk of orofacial clefts.
Prednisolone can cause fetal harm when used in pregnancy. RAYOS should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. If this drug is used during pregnancy, or if the patient becomes pregnant while using this drug, the patient should be apprised of the potential hazard to the fetus. Infants born to mothers who have received substantial doses of corticosteroids during pregnancy should be carefully observed for signs of hypoadrenalism.
Nursing Mothers
Prednisolone, the active metabolite of prednisone, is secreted in human milk. Reports suggest that prednisolone concentrations in human milk are 5 to 25% of maternal serum levels, and that total infant daily doses are small, about 0.14% of the maternal daily dose. The risk of infant exposure to prednisolone through breast milk should be weighed against the known benefits of breastfeeding for both the mother and baby.
Caution should be exercised when RAYOS is administered to a nursing woman. If RAYOS must be prescribed to a breastfeeding mother, the lowest dose should be prescribed to achieve the desired clinical effect. High doses of corticosteroids for long periods could potentially produce problems in infant growth and development and interfere with endogenous corticosteroid production.
Pediatric Use
The efficacy and safety of prednisone in the pediatric population are based on the well-established course of effect of corticosteroids which is similar in pediatric and adult populations. Published studies provide evidence of efficacy and safety in pediatric patients for the treatment of nephrotic syndrome ( > 2 years of age), and aggressive lymphomas and leukemias ( > 1 month of age). However, some of these conclusions and other indications for pediatric use of corticosteroid, e.g., severe asthma and wheezing, are based on adequate and well-controlled trials conducted in adults, on the premises that the course of the diseases and their pathophysiology are considered to be substantially similar in both populations. The adverse effects of prednisone in pediatric patients are similar to those in adults. Like adults, pediatric patients should be carefully observed with frequent measurements of blood pressure, weight, height, intraocular pressure, and clinical evaluation for the presence of infection, psychosocial disturbances, thromboembolism, peptic ulcers, cataracts, and osteoporosis.
Children who are treated with corticosteroids by any route, including systemically administered corticosteroids, may experience a decrease in their growth velocity. This negative impact of corticosteroids on growth has been observed at low systemic doses and in the absence of laboratory evidence of HPA axis suppression (i.e., cosyntropin stimulation and basal cortisol levels). Growth velocity may therefore be a more sensitive indicator of systemic corticosteroid exposure in children than some commonly used tests of HPA axis function. The linear growth of children treated with corticosteroids by any route should be monitored, and the potential growth effects of prolonged treatment should be weighed against clinical benefits obtained and the availability of other treatment alternatives. In order to minimize the potential growth effects of corticosteroids, children should be titrated to the lowest effective dose
Geriatric Use
No overall differences in safety or effectiveness were observed between elderly subjects and younger subjects, and other reported clinical experience with prednisone has not identified differences in responses between the elderly and younger patients. However, the incidence of corticosteroid-induced side effects may be increased in geriatric patients and are dose-related. Osteoporosis is the most frequently encountered complication, which occurs at a higher incidence rate in corticosteroid-treated geriatric patients as compared to younger populations and in age-matched controls. Losses of bone mineral density appear to be greatest early on in the course of treatment and may recover over time after steroid withdrawal or use of lower doses (i.e., ≥ 5 mg/day). Prednisone doses of 7.5 mg/day or higher have been associated with an increased relative risk of both vertebral and nonvertebral fractures, even in the presence of higher bone density compared to patients with involution osteoporosis. Routine screening of geriatric patients, including regular assessments of bone mineral density and institution of fracture prevention strategies, along with regular review of prednisone indication should be undertaken to minimize complications and keep the prednisolone dose at the lowest acceptable level. CoÂadministration of certain bisphosphonates have been shown to retard the rate of bone loss in corticosteroid-treated males and postmenopausal females, and these agents are recommended in the prevention and treatment of corticosteroid-induced osteoporosis.
It has been reported that equivalent weight-based doses yield higher total and unbound prednisolone plasma concentrations and reduced renal and non-renal clearance in elderly patients compared to younger populations. Dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
Care should be taken to ensure that the eye is not infected before Minims Prednisolone is used.
Systemic absorption may be reduced by compressing the lacrimal sac at the medial canthus for a minute during and following the instillation of the drops. (This blocks the passage of drops via the naso-lacrimal duct to the wide absorptive area of the nasal and pharyngeal mucosa. It is especially advisable in children.).
Visual disturbance
Visual disturbance may be reported with systemic and topical corticosteroid use. If a patient presents with symptoms such as blurred vision or other visual disturbances, the patient should be considered for referral to an ophthalmologist for evaluation of possible causes which may include cataract, glaucoma or rare diseases such as central serous chorioretinopathy (CSCR) which have been reported after use of systemic and topical corticosteroids.
WARNINGS
Included as part of the PRECAUTIONS section.
PRECAUTIONS
Alterations in Endocrine Function
Hypothalamic-pituitary-adrenal (HPA) axis suppression, Cushing’s syndrome, and hyperglycemia. Monitor patients for these conditions with chronic use.
Corticosteroids can produce reversible hypothalamic-pituitary adrenal (HPA) axis suppression with the potential for corticosteroid insufficiency after withdrawal of treatment. Drug-induced secondary adrenocortical insufficiency may be minimized by gradual reduction of dosage. This type of relative insufficiency may persist for months after discontinuation of therapy; therefore, in any situation of stress occurring during that period, hormone therapy should be reinstituted. If the patient is receiving corticosteroids already, dosage may have to be increased.
Since mineralocorticoid secretion may be impaired, salt and/or a mineralocorticoid should be administered concurrently. Mineralocorticoid supplementation is of particular importance in infancy.
Metabolic clearance of corticosteroids is decreased in hypothyroid patients and increased in hyperthyroid patients. Changes in thyroid status of the patient may necessitate adjustment in dosage.
Increased Risks Related to Infection
Corticosteroids may increase the risks related to infections with any pathogen, including viral, bacterial, fungal, protozoan, or helminthic infections. The degree to which the dose, route and duration of corticosteroid administration correlates with the specific risks of infection is not well characterized, however, with increasing doses of corticosteroids, the rate of occurrence of infectious complications increases.
Corticosteroids may mask some signs of infection and may reduce resistance to new infections.
Corticosteroids may exacerbate infections and increase risk of disseminated infections.
The use of prednisone in active tuberculosis should be restricted to those cases of fulminating or disseminated tuberculosis in which the corticosteroid is used for management of the disease in conjunction with an appropriate anti-tuberculous regimen.
Chickenpox and measles can have a more serious or even fatal course in non-immune children or adults on corticosteroids. In children or adults who have not had these diseases, particular care should be taken to avoid exposure. If a patient is exposed to chickenpox, prophylaxis with varicella zoster immune globulin (VZIG) may be indicated. If patient is exposed to measles, prophylaxis with pooled intramuscular immunoglobulin (IG) may be indicated. If chickenpox develops, treatment with antiviral agents may be considered.
Corticosteroids should be used with great care in patients with known or suspected Strongyloides (threadworm) infestation. In such patients, corticosteroid-induced immunosuppression may lead to Strongyloides hyperinfection and dissemination with widespread larval migration, often accompanied by severe enterocolitis and potentially fatal gram-negative septicemia.
Corticosteroids may exacerbate systemic fungal infections and therefore should not be used in the presence of such infections unless they are needed to control drug reactions.
Corticosteroids may increase risk of reactivation or exacerbation of latent infection.
If corticosteroids are indicated in patients with latent tuberculosis or tuberculin reactivity, close observation is necessary as reactivation of the disease may occur. During prolonged corticosteroid therapy, these patients should receive chemoprophylaxis.
Corticosteroids may activate latent amebiasis. Therefore, it is recommended that latent amebiasis or active amebiasis be ruled out before initiating corticosteroid therapy in any patient who has spent time in the tropics or any patient with unexplained diarrhea.
Corticosteroids should not be used in cerebral malaria.
Alterations in Cardiovascular/Renal Function
Corticosteroids can cause elevation of blood pressure, salt, and water retention, and increased excretion of potassium and calcium. These effects are less likely to occur with the synthetic derivatives except when used in large doses. Dietary salt restriction and potassium supplementation may be necessary. These agents should be used with caution in patients with congestive heart failure, hypertension, or renal insufficiency.
Literature reports suggest an apparent association between use of corticosteroids and left ventricular free wall rupture after a recent myocardial infarction; therefore, therapy with corticosteroids should be used with great caution in these patients.
Use in Patients with Gastrointestinal Disorders
There is an increased risk of gastrointestinal perforation in patients with certain GI disorders. Signs of GI perforation, such as peritoneal irritation may be masked in patients receiving corticosteroids.
Corticosteroids should be used with caution if there is a probability of impending perforation, abscess, or other pyogenic infections; diverticulitis; fresh intestinal anastomoses; and active or latent peptic ulcer.
Behavioral and Mood Disturbances
Corticosteroids use may be associated with central nervous system effects ranging from euphoria, insomnia, mood swings, personality changes, and severe depression, to frank psychotic manifestations. Also, existing emotional instability or psychotic tendencies may be aggravated by corticosteroids.
Decrease in Bone Density
Corticosteroids decrease bone formation and increase bone resorption both through their effect on calcium regulation (i.e., decreasing absorption and increasing excretion) and inhibition of osteoblast function. This, together with a decrease in the protein matrix of the bone secondary to an increase in protein catabolism, and reduced sex hormone production, may lead to inhibition of bone growth in children and adolescents and the development of osteoporosis at any age. Special consideration should be given to patients at increased risk of osteoporosis (i.e., postmenopausal women) before initiating corticosteroid therapy and bone density should be monitored in patients on long term corticosteroid therapy.
Ophthalmic Effects
Prolonged use of corticosteroids may produce posterior subcapsular cataracts, glaucoma with possible damage to the optic nerves, and may enhance the establishment of secondary ocular infections due to fungi or viruses.
The use of oral corticosteroids is not recommended in the treatment of optic neuritis and may lead to an increase in the risk of new episodes.
Intraocular pressure may become elevated in some individuals. If corticosteroid therapy is continued for more than 6 weeks, intraocular pressure should be monitored.
Corticosteroids should be used cautiously in patients with ocular herpes simplex because of possible corneal perforation. Corticosteroids should not be used in active ocular herpes simplex.
Vaccination
Administration of live or live, attenuated vaccines is contraindicated in patients receiving immunosuppressive doses of corticosteroids. Killed or inactivated vaccines may be administered; however, the response to such vaccines cannot be predicted. Immunization procedures may be undertaken in patients who are receiving corticosteroids as replacement therapy, e.g., for Addison’s disease.
While on corticosteroid therapy, patients should not be vaccinated against smallpox. Other immunization procedures should not be undertaken in patients who are on corticosteroids, especially on high dose, because of possible hazards of neurological complications and a lack of antibody response.
Effect on Growth and Development
Long-term use of corticosteroids can have negative effects on growth and development in children.
Growth and development of pediatric patients on prolonged corticosteroid therapy should be carefully monitored.
Use in Pregnancy
Prednisone can cause fetal harm when administered to a pregnant woman. Human and animal studies suggest that use of corticosteroids during the first trimester of pregnancy is associated with an increased risk of orofacial clefts, intrauterine growth restriction, and decreased birth weight. If this drug is used during pregnancy, or if the patient becomes pregnant while using this drug, the patient should be apprised of the potential hazard to the fetus.
Neuromuscular Effects
Although controlled clinical trials have shown corticosteroids to be effective in speeding the resolution of acute exacerbations of multiple sclerosis, they do not show that they affect the ultimate outcome or natural history of the disease. The studies do show that relatively high doses of corticosteroids are necessary to demonstrate a significant effect.
An acute myopathy has been observed with the use of high doses of corticosteroids, most often occurring in patients with disorders of neuromuscular transmission (e.g., myasthenia gravis), or in patients receiving concomitant therapy with neuromuscular blocking drugs (e.g., pancuronium). This acute myopathy is generalized, may involve ocular and respiratory muscles, and may result in quadriparesis. Elevation of creatine kinase may occur. Clinical improvement or recovery after stopping corticosteroids may require weeks to years.
Kaposi’s Sarcoma
Kaposi’s sarcoma has been reported to occur in patients receiving corticosteroid therapy, most often for chronic conditions. Discontinuation of corticosteroids may result in clinical improvement.
Nonclinical Toxicology
Carcinogenesis, Mutagenesis, Impairment of Fertility
Prednisone was not formally evaluated in carcinogenicity studies. Review of the published literature identified carcinogenicity studies of prednisolone, the active metabolite of prednisone, at doses which were less than the typical clinical doses. In a 2-year study, male Sprague-Dawley rats administered prednisolone in drinking water at a dose of 368 mcg/kg/day (equivalent to 3.5 mg/day in a 60-kg individual based on a mg/m² body surface area comparison) developed increased incidences of hepatic adenomas. Lower doses were not studied, and therefore, a no effect level could not be identified. In an 18-month study, intermittent oral gavage administration of prednisolone did not induce tumors in female Sprague-Dawley rats when given 1, 2, 4.5, or 9 times per month at 3 mg/kg prednisone (equivalent to 29 mg in a 60-kg individual based on a mg/m² body surface area comparison).
Prednisone was not formally evaluated for genotoxicity. However, in published studies prednisolone was not mutagenic with or without metabolic activation in the Ames bacterial reverse mutation assay using Salmonella typhimurium and Escherichia coli, or in a mammalian cell gene mutation assay using mouse lymphoma L5178Y cells, according to current evaluation standards. In a published chromosomal aberration study in Chinese Hamster Lung (CHL) cells, a slight increase was seen in the incidence of structural chromosomal aberrations with metabolic activation at the highest concentration tested, however, the effect appears to be equivocal. Prednisolone was not genotoxic in an in vivo micronucleaus assay in the mouse, though the study design did not meet current criteria.
Prednisone was not formally evaluated in fertility studies. However, menstrual irregularities have been described with clinical use.
Use In Specific Populations
Pregnancy
Teratogenic Effects
Pregnancy Category D : Multiple cohort and case controlled studies in humans suggest that maternal corticosteroid use during the first trimester increases the rate of cleft lip with or without cleft palate from about 1/1000 infants to 3-5/1000 infants. Two prospective case control studies showed decreased birth weight in infants exposed to maternal corticosteroids in utero.
Estilsona was not formally evaluated for effects on reproduction. Published literature indicates prednisolone, the active metabolite of prednisone, has been shown to be teratogenic in rats, rabbits, hamsters, and mice with increased incidence of cleft palate in offspring. In teratogenicity studies, cleft palate along with elevation of fetal lethality (or increase in resorptions) and reductions in fetal body weight were seen in rats at maternal doses of 30 mg/kg (equivalent to 290 mg in a 60 kg individual based on mg/m² body surface comparison) and higher. Cleft palate was observed in mice at a maternal dose of 20 mg/kg (equivalent to 100 mg in a 60 kg individual based on mg/m² comparison). Additionally, constriction of the ductus arteriosus has been observed in fetuses of pregnant rats exposed to prednisolone.
In humans, the risk of decreased birth weight appears to be dose related and may be minimized by administering lower corticosteroid doses. It is likely that underlying maternal conditions contribute to intrauterine growth restriction and decreased birth weight, but it is unclear to what extent these maternal conditions contribute to the increased risk of orofacial clefts.
Prednisolone can cause fetal harm when used in pregnancy. Estilsona should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. If this drug is used during pregnancy, or if the patient becomes pregnant while using this drug, the patient should be apprised of the potential hazard to the fetus. Infants born to mothers who have received substantial doses of corticosteroids during pregnancy should be carefully observed for signs of hypoadrenalism.
Nursing Mothers
Prednisolone, the active metabolite of prednisone, is secreted in human milk. Reports suggest that prednisolone concentrations in human milk are 5 to 25% of maternal serum levels, and that total infant daily doses are small, about 0.14% of the maternal daily dose. The risk of infant exposure to prednisolone through breast milk should be weighed against the known benefits of breastfeeding for both the mother and baby.
Caution should be exercised when Estilsona is administered to a nursing woman. If Estilsona must be prescribed to a breastfeeding mother, the lowest dose should be prescribed to achieve the desired clinical effect. High doses of corticosteroids for long periods could potentially produce problems in infant growth and development and interfere with endogenous corticosteroid production.
Pediatric Use
The efficacy and safety of prednisone in the pediatric population are based on the well-established course of effect of corticosteroids which is similar in pediatric and adult populations. Published studies provide evidence of efficacy and safety in pediatric patients for the treatment of nephrotic syndrome ( > 2 years of age), and aggressive lymphomas and leukemias ( > 1 month of age). However, some of these conclusions and other indications for pediatric use of corticosteroid, e.g., severe asthma and wheezing, are based on adequate and well-controlled trials conducted in adults, on the premises that the course of the diseases and their pathophysiology are considered to be substantially similar in both populations. The adverse effects of prednisone in pediatric patients are similar to those in adults. Like adults, pediatric patients should be carefully observed with frequent measurements of blood pressure, weight, height, intraocular pressure, and clinical evaluation for the presence of infection, psychosocial disturbances, thromboembolism, peptic ulcers, cataracts, and osteoporosis.
Children who are treated with corticosteroids by any route, including systemically administered corticosteroids, may experience a decrease in their growth velocity. This negative impact of corticosteroids on growth has been observed at low systemic doses and in the absence of laboratory evidence of HPA axis suppression (i.e., cosyntropin stimulation and basal cortisol levels). Growth velocity may therefore be a more sensitive indicator of systemic corticosteroid exposure in children than some commonly used tests of HPA axis function. The linear growth of children treated with corticosteroids by any route should be monitored, and the potential growth effects of prolonged treatment should be weighed against clinical benefits obtained and the availability of other treatment alternatives. In order to minimize the potential growth effects of corticosteroids, children should be titrated to the lowest effective dose
Geriatric Use
No overall differences in safety or effectiveness were observed between elderly subjects and younger subjects, and other reported clinical experience with prednisone has not identified differences in responses between the elderly and younger patients. However, the incidence of corticosteroid-induced side effects may be increased in geriatric patients and are dose-related. Osteoporosis is the most frequently encountered complication, which occurs at a higher incidence rate in corticosteroid-treated geriatric patients as compared to younger populations and in age-matched controls. Losses of bone mineral density appear to be greatest early on in the course of treatment and may recover over time after steroid withdrawal or use of lower doses (i.e., ≥ 5 mg/day). Prednisone doses of 7.5 mg/day or higher have been associated with an increased relative risk of both vertebral and nonvertebral fractures, even in the presence of higher bone density compared to patients with involution osteoporosis. Routine screening of geriatric patients, including regular assessments of bone mineral density and institution of fracture prevention strategies, along with regular review of prednisone indication should be undertaken to minimize complications and keep the prednisolone dose at the lowest acceptable level. CoÂadministration of certain bisphosphonates have been shown to retard the rate of bone loss in corticosteroid-treated males and postmenopausal females, and these agents are recommended in the prevention and treatment of corticosteroid-induced osteoporosis.
It has been reported that equivalent weight-based doses yield higher total and unbound prednisolone plasma concentrations and reduced renal and non-renal clearance in elderly patients compared to younger populations. Dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
A prednisone-based pharmacotherapy should only be given when absolutely necessary and should be accompanied by appropriate anti-infectious therapy in the presence of the following conditions:
— Acute viral infections (herpes zoster, herpes simplex, varicella, herpetic keratitis),
— HBsAg-positive chronic active hepatitis,
— Approximately 8 weeks before and 2 weeks after immunisation with live vaccines,
— Systemic mycoses and parasitoses (e.g. nematodes),
— Poliomyelitis,
— Lymphadenitis following BCG inoculation,
— Acute and chronic bacterial infections,
— History of tuberculosis (caution: reactivation!) Due to their immunosuppressive properties glucocorticoids can induce or aggravate infections. Such patients should be monitored carefully e.g. by performing a tuberculin test. Patients at special risk should receive a tuberculostatic treatment.
In addition, a prednisone-based pharmacotherapy should only be given when necessary and should be accompanied if required by appropriate therapy in the presence of the following conditions:
— Gastrointestinal ulcers,
— Severe osteoporosis and osteomalacia
— Hypertension that is difficult to control,
— Severe diabetes mellitus,
— Psychiatric disorders (also if in patient’s history),
— Narrow- and wide-angle glaucoma,
— Corneal ulcers and corneal injuries.
Because of the risk of intestinal perforation, prednisone may only be used if absolutely necessary and with adequate monitoring in cases of:
— Severe ulcerative colitis with imminent perforation,
— Diverticulitis,
— Entero-anastomoses (immediately postoperative).
Visual disturbance
Visual disturbance may be reported with systemic and topical corticosteroid use. If a patient presents with symptoms such as blurred vision or other visual disturbances, the patient should be considered for referral to an ophthalmologist for evaluation of possible causes which may include cataract, glaucoma or rare diseases such as central serous chorioretinopathy (CSCR) which have been reported after use of systemic and topical corticosteroids.
Scleroderma renal crisis
Caution is required in patients with systemic sclerosis because of an increased incidence of (possibly fatal) scleroderma renal crisis with hypertension and decreased urinary output observed with a daily dose of 15 mg or more prednisolone. Blood pressure and renal function (s-creatinine) should therefore be routinely checked. When renal crisis is suspected, blood pressure should be carefully controlled.
Lodotra cannot achieve the desired blood concentration of prednisone if taken under fasting conditions. Therefore, Lodotra should always be taken with or after the evening meal in order to ensure sufficient efficacy. In addition, low plasma concentrations may occur in 6% -7% of Lodotra doses as observed across all pharmacokinetic studies and 11% in a single pharmacokinetic study when taken according to the recommendations. This should be considered if Lodotra is not sufficiently effective. In these situations a switch to a conventional immediate-release formulation may be considered.
Lodotra should not be substituted by prednisone immediate-release tablets in the same administration regime because of Lodotra‘s delayed release mechanism.
In case of substitution, termination, or discontinuing prolonged treatment, the following risks must be considered: Recurrence of the rheumatoid arthritis disease activity, acute adrenal failure (especially in stressful situations, e. g. during infections, after accidents, with increased physical strain), cortisone withdrawal syndrome.
Lodotra should not be given as for acute indications instead of prednisone immediate-release tablets due to its pharmacological properties.
During the use of Lodotra, a possibly increased need for insulin or oral anti-diabetics should be considered. Patients with diabetes mellitus should therefore be treated under close monitoring.
During the treatment with Lodotra, regular blood pressure checks are required in patients with hypertension that is difficult to control.
Patients with severe cardiac insufficiency have to be closely monitored because of the risk of deterioration of the condition.
Caution is necessary when corticosteroids, including prednisone, are prescribed to a patient with recent myocardial infarction due to a risk of myocardial rupture.
Caution is necessary when corticosteroids, including prednisone, are prescribed to patients with renal insufficiency.
Sleep disorder is documented to occur more frequently with Lodotra than with conventional immediate release formulations which are taken in the morning. If insomnia occurs and does not improve, a switch to a conventional immediate release formulation may be advisable.
The treatment with Lodotra can also mask signs and symptoms of an existing or developing infection and thus may render diagnostic efforts more difficult.
Even with low doses, long-term use of Lodotra results in an increased risk of infection. These possible infections may also be brought about by microorganisms that rarely cause infection under normal circumstances (so-called opportunistic infections).
Certain viral diseases (varicella, measles) may take a more severe course in patients treated with glucocorticoids. Immunosuppressed individuals without prior varicella or measles infection are at particular risk. If such individuals, while being treated with Lodotra, have contact with persons infected with varicella or measles, a preventive treatment should be initiated, if required.
In patients with known or suspected Strongyloids (threadworm) infestation glucocorticoids may lead to Strongyloides hyperinfection and dissemination with widespread larval migration.
Vaccinations with inactivated vaccines are generally possible. However, it has to be taken into account that the immune response and consequently the success of the vaccination may be impaired with higher doses of glucocorticoids.
In case of long-term therapy with Lodotra, regular medical follow-ups (including ophthalmologic examinations at three month intervals) are indicated; if comparatively high doses are given, sufficient supply of potassium supplements and restriction of sodium have to be ensured and serum potassium levels have to be monitored.
If during the treatment with Lodotra high levels of physical stress are caused by certain events (accidents, surgical procedure etc.), a temporary dose increase may become necessary.
Depending on the duration of the treatment and the dosage used, a negative impact on calcium metabolism must be expected. Osteoporosis prophylaxis is therefore recommended and is particularly important if other risk factors are present (including familial predisposition, advanced age, postmenopausal status, insufficient intake of protein and calcium, excessive smoking, excessive alcohol consumption, as well as reduced physical activity). The prophylaxis is based on a sufficient supply of calcium and vitamin D, as well as on physical activity. In case of pre-existing osteoporosis, an additional therapy should be considered.
The medicinal product contains lactose monohydrate. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
When using high doses of prednisolone for an extended period of time (30 mg/day for a minimum of 4 weeks), reversible disturbances of spermatogenesis were observed that persisted for several months after discontinuation of the medicinal product.
WARNINGS
Prolonged use of corticosteroids may result in posterior subcapsular cataract formation and may increase intraocular pressure in susceptible individuals, resulting in glaucoma with damage to the optic nerve, defects in visual acuity and fields of vision. Prolonged use may also suppress the host immune response and thus increase the hazard of secondary ocular infections.
If this product is used for 10 days or longer, intraocular pressure should be routinely monitored even though it may be difficult in children and uncooperative patients. Steroids should be used with caution in the presence of glaucoma. Intraocular pressure should be checked frequently. Various ocular diseases and long-term use of topical corticosteroids have been known to cause corneal and scleral thinning. Use of topical corticosteroids in the presence of thin corneal or scleral tissue may lead to perforation.
Acute purulent infections of the eye may be masked or activity enhanced by the presence of corticosteroid medication.
The use of steroids after cataract surgery may delay healing and increase the incidence of bleb formation.
Use of ocular steroids may prolong the course and may exacerbate the severity of many viral infections of the eye (including herpes simplex). Employment of a corticosteroid medication in the treatment of patients with a history of herpes simplex requires great caution; frequent slit lamp microscopy is recommended.
Estilsona® suspension contains sodium bisulfite, a sulfite that may cause allergic-type reactions, including anaphylactic symptoms and life-threatening or less severe asthmatic episodes in certain susceptible people. The overall prevalence of sulfite sensitivity in the general population is unknown and probably low. Sulfite sensitivity is seen more frequently in asthmatic than in non-asthmatic people.
PRECAUTIONS
General
The initial prescription and renewal of the medication order beyond 20 milliliters of PRED FORTE® suspension should be made by a physician only after examination of the patient with the aid of magnification, such as slit lamp biomicroscopy, and, where appropriate, fluorescein staining. If signs and symptoms fail to improve after 2 days, the patient should be re-evaluated.
As fungal infections of the cornea are particularly prone to develop coincidentally with longterm local corticosteroid applications, fungal invasion should be suspected in any persistent corneal ulceration where a corticosteroid has been used or is in use. Fungal cultures should be taken when appropriate.
Carcinogenesis, Mutagenesis, Impairment Of Fertility
No studies have been conducted in animals or in humans to evaluate the potential of these effects.
Pregnancy
Prednisolone has been shown to be teratogenic in mice when given in doses 1-10 times the human dose. Dexamethasone, hydrocortisone, and prednisolone were ocularly applied to both eyes of pregnant mice five times per day on days 10 through 13 of gestation. A significant increase in the incidence of cleft palate was observed in the fetuses of the treated mice. There are no adequate well-controlled studies in pregnant women. Prednisolone should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Nursing Mothers
It is not known whether topical ophthalmic administration of corticosteroids could result in sufficient systemic absorption to produce detectable quantities in breast milk. Systemically administered corticosteroids appear in human milk and could suppress growth, interfere with endogenous corticosteroid production, or cause other untoward effects. Because of the potential for serious adverse reactions in nursing infants from prednisolone, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
The safety and effectiveness in pediatric patients have been established. Use in pediatric patients is supported by evidence from adequate and well-controlled studies of prednisolone acetate ophthalmic suspension in adults with additional data in pediatric patients.
Geriatric Use
No overall differences in safety or effectiveness have been observed between elderly and younger patients.

Prednisolone (Estilsona)
Prednisolone is used for treating allergies, arthritis, breathing problems (eg, asthma), certain blood disorders, collagen diseases (eg, lupus), certain eye diseases (eg, keratitis), cancer (eg, leukemia), endocrine problems (eg, adrenocortical insufficiency), intestinal problems (eg, ulcerative colitis), swelling due to certain conditions, or skin conditions (eg, psoriasis).
Other names for this medication:
Adelcort, Adelone, Aersolin d, Ak-pred, Alertine, Alpicort, Apicort, Aprednislon, Bisuo a, Blephamide, Bronal, Capsoid, Cetapred, Chloramphecort-h, Compesolon, Cor tyzine, Corotrope, Cortan, Cortico-sol, Cortisal, Cortisol, Danalone, Decortin h, Delta-cortef, Deltacortenesol, Deltacortril, Deltahydrocortisone, Deltapred, Deltastab, Dermol, Dermosolon, Deturgylone, Dhasolone, Di-adreson-f, Dojilon, Dontisolon, Econopred, Emsolone, Encortolon, Estilsona, Fenicort, Fisiopred, Fisopred, Flo-pred, Frisolona forte, Glucortin, Gupisone, Hefasolon, Hexacorton, Hexy-solupred, Hydrocortancyl, Hydrocortidelt, Infectocortikrupp, Inflanefran, Inflanegent, Insolone, Intalsolone, Key-pred, Klismacort, Kohakusanin, Lenisolone, Lepicortinolo, Lidomex kowa, Linola-h n, Locaseptil-neo, Lygal, Mecortolon, Mediasolone, Medopred, Meprisolon, Metacortandralone, Meti-derm, Meticortelone, Minisolone, Nurisolon, Ocupred, Oftalmol, Omnipred, Ophtapred, Optipred, Optival, Orapred, Orapred odt, Panafcortelone, Paracortol, Parisilon, Pediacort, Pediapred, Pednisol, Precodil, Precortalon aquosum, Pred-clysma, Predacort, Predalone, Predate s, Predcor, Predenema, Predfoam, Predicort, Predinga, Predlone, Predmix, Prednefrin, Prednesol, Predni, Predni h tablinen, Predni-pos, Prednicortil, Prednigalen, Prednihexal, Predniliderm, Predniocil, Prednip, Prednis, Prednisolon caproate, Prednisolona, Prednisolonacetat, Prednisolonpivalat, Prednisolonum, Prednisolut, Prednizolons, Predohan, Predonema, Predonine, Predsim, Predsol, Predsolets, Preflam, Prelon, Prelone, Premandol, Prenin, Prenolone, Preson, Prezolon, Rectopred, Redipred, Riemser, Scheriproct, Scherisolona, Sintisone, Solone, Solpren, Solu-dacortina, Solu-decortin, Soluble prednisolone, Solupred, Sopacortelone, Sophipren, Spirazon, Spiricort, Sterolone, Ultracortenol, Vasocidin, Walesolone, Wysolone, Youmeton
Show all
-
INDICATIONS
Prednisolone is used for treating allergies, arthritis, breathing problems (eg, asthma), certain blood disorders, collagen diseases (eg, lupus), certain eye diseases (eg, keratitis), cancer (eg, leukemia), endocrine problems (eg, adrenocortical insufficiency), intestinal problems (eg, ulcerative colitis), swelling due to certain conditions, or skin conditions (eg, psoriasis). Prednisolone is a corticosteroid. It works by modifying the body’s immune response to various conditions and decreasing inflammation.
INSTRUCTIONS
Use Prednisolone as directed by your doctor.
- Take Prednisolone by mouth with food.
- If you miss a dose of Prednisolone, take it as soon as possible. If it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not take 2 doses at once.
Ask your health care provider any questions you may have about how to use Prednisolone.
STORAGE
Store Prednisolone at room temperature, between 68 and 77 degrees F (20 and 25 degrees C), in a tightly closed container. Store away from heat, moisture, and light. Do not store in the bathroom. Keep Prednisolone out of the reach of children and away from pets.
-
Do NOT use Prednisolone if:
- you are allergic to any ingredient in Prednisolone
- you have a systemic fungal infection, a certain type of malaria, inflammation of the optic nerve, or herpes infection of the eye
- you are scheduled to have a live or attenuated live vaccination (eg, smallpox)
- you are taking mifepristone.
Contact your doctor right away if any of these apply to you.
Some medical conditions may interact with Prednisolone. Tell your doctor or pharmacist if you have any medical conditions, especially if any of the following apply to you:
- if you are pregnant, planning to become pregnant, or are breast-feeding
- if you are taking any prescription or nonprescription medicine, herbal preparation, or dietary supplement
- if you have allergies to medicines, foods, or other substances
- if you have a history of heart problems (eg, congestive heart failure), heart attack, high blood pressure, kidney problems, liver problems, diabetes, seizures, an underactive thyroid, adrenal gland problems, fluid retention (eg, swelling of the hands, ankles, or feet), or any mental or mood problems
- if you have or have recently had a fungal, bacterial, viral, or other type of infection; herpes infection of the eye; chickenpox; measles; or shingles
- if you have HIV infection or tuberculosis (TB) infection, or if you have had ever had a positive TB skin test
- if you have any stomach problems (eg, ulcers), intestinal problems (eg, blockage, perforation, or infection; unexplained diarrhea; diverticulitis; ulcerative colitis), recent intestinal surgery, or inflammation of the esophagus
- if you have weak bones (eg, osteoporosis) or muscle problems (eg, myasthenia gravis)
- if you have had a recent vaccination (eg, smallpox).
Some medicines may interact with Prednisolone. Tell your health care provider if you are taking any other medicines, especially any of the following:
- Clarithromycin, cyclosporine, estrogens (eg, estradiol), oral contraceptives (eg, birth control pills), or ketoconazole because they may increase the risk of Prednisolone’s side effects
- Barbiturates (eg, phenobarbital), carbamazepine, ephedrine, hydantoins (eg, phenytoin), or rifampin because they may decrease Prednisolone’s effectiveness
- Anticholinesterases (eg, pyridostigmine), aspirin, diuretics (eg, hydrochlorothiazide, furosemide), methotrexate, mifepristone, quinolone antibiotics (eg, ciprofloxacin), ritodrine, or live or attenuated live vaccines because the risk of their side effects may be increased by Prednisolone
- Anticoagulants (eg, warfarin), hydantoins (eg, phenytoin), or killed or inactivated vaccines because their effectiveness may be decreased by Prednisolone.
This may not be a complete list of all interactions that may occur. Ask your health care provider if Prednisolone may interact with other medicines that you take. Check with your health care provider before you start, stop, or change the dose of any medicine.
Important safety information:
- Avoid alcohol while you are using Prednisolone.
- Prednisolone may lower the ability of your body to fight infection. Avoid contact with people who have colds or infections. Tell your doctor if you notice signs of infection like fever, sore throat, rash, or chills.
- If you have not had chickenpox, shingles, or measles, avoid contact with anyone who does.
- If you are taking Prednisolone regularly over a long period of time, carry an ID card at all times that says you take Prednisolone.
- Do not receive a live vaccine (eg, measles, mumps, smallpox) while you are taking Prednisolone. Talk with your doctor before you receive any vaccine.
- Tell your doctor or dentist that you take Prednisolone before you receive any medical or dental care, emergency care, or surgery.
- Diabetes patients — Prednisolone may affect your blood sugar. Check blood sugar levels closely. Ask your doctor before you change the dose of your diabetes medicine.
- Lab tests, including adrenal function tests, may be performed while you use Prednisolone. These tests may be used to monitor your condition or check for side effects. Be sure to keep all doctor and lab appointments.
- Caution is advised when using Prednisolone in children; they may be more sensitive to its effects.
- Corticosteroids may affect growth rate in children and teenagers in some cases. They may need regular growth checks while they take Prednisolone.
- Pregnancy and breast-feeding: If you become pregnant, contact your doctor. You will need to discuss the benefits and risks of using Prednisolone while you are pregnant. Prednisolone is found in breast milk. If you are or will be breast-feeding while you use Prednisolone, check with your doctor. Discuss any possible risks to your baby.
If you are on long-term or high dosage therapy and you suddenly stop taking Prednisolone, you may have withdrawal symptoms, including fever, vomiting, appetite loss, diarrhea, nausea, dizziness, weight loss, weakness, general body discomfort, joint or muscle pain.
-
All medicines may cause side effects, but many people have no, or minor, side effects.
Check with your doctor if any of these most common side effects persist or become bothersome:
Acne; clumsiness; dizziness; facial flushing; feeling of a whirling motion; general body discomfort; headache; increased appetite; increased sweating; nausea; nervousness; sleeplessness; upset stomach.
Seek medical attention right away if any of these severe side effects occur:
Severe allergic reactions (rash; hives; itching; difficulty breathing; tightness in the chest; swelling of the mouth, face, lips, or tongue); black, tarry stools; changes in body fat; changes in menstrual period; changes in skin color; chest pain; easy bruising or bleeding; increased hunger, thirst, or urination; mental or mood changes (eg, depression); muscle pain, weakness, or wasting; seizures; severe nausea or vomiting; shortness of breath; signs of infection (eg, fever, chills, persistent sore throat); sudden severe dizziness or headache; swelling of ankles, feet, or hands; tendon or bone pain; thinning of skin; unusual skin sensation; unusual weight gain; vision changes or other eye problems; vomit that looks like coffee grounds.
This is not a complete list of all side effects that may occur. If you have questions about side effects, contact your health care provider.

Описание препарата СОМНОЛ® (таблетки, покрытые пленочной оболочкой, 7.5 мг) основано на официальной инструкции, утверждено компанией-производителем в 2017 году
Дата согласования: 25.09.2017
Содержание
- Фотографии упаковок
- Действующее вещество
- ATX
- Фармакологическая группа
- Нозологическая классификация (МКБ-10)
- Состав
- Описание лекарственной формы
- Фармакологическое действие
- Фармакодинамика
- Фармакокинетика
- Показания
- Противопоказания
- Применение при беременности и кормлении грудью
- Способ применения и дозы
- Побочные действия
- Взаимодействие
- Передозировка
- Особые указания
- Форма выпуска
- Производитель
- Условия отпуска из аптек
- Условия хранения
- Срок годности
- Аналоги (синонимы) препарата СОМНОЛ®
- Заказ в аптеках Москвы
Фотографии упаковок

25.09.2017
Действующее вещество
ATX
Фармакологическая группа
Состав
| Таблетки, покрытые пленочной оболочкой | 1 табл. |
| активное вещество: | |
| зопиклон | 7,5 мг |
| вспомогательные вещества: кальция гидрофосфат безводный — 152,3 мг; крахмал картофельный высушенный — 4,25 мг; магния стеарат — 1,7 мг; карбоксиметилкрахмал натрия — 1,7 мг; кремния диоксид — 2,55 мг | |
| оболочка пленочная: Opadry 33G28707 белый (гипромеллоза — 40%, лактозы моногидрат — 24%, макрогол 3000 — 22%, титана диоксид — 8%, триацетин — 6%) — 2,6 мг |
Описание лекарственной формы
Круглые таблетки, покрытые пленочной оболочкой белого цвета, с одной стороны выпуклые, с другой — вогнутые с риской.
Фармакологическое действие
Фармакологическое действие
—
снотворное.
Фармакодинамика
Зопиклон является снотворным средством группы циклопирролонов, структурно отличающихся от бензодиазепинов и барбитуратов. Он обладает следующими фармакологическими свойствами: снотворным, седативным, транквилизирующим, противосудорожным и миорелаксирующим. Эти эффекты зопиклона связаны со специфическим агонистическим действием на рецепторы ЦНС, относящиеся к макромолекулярному комплексу ГАМК-омега, модулирующему открытие нейрональных каналов для ионов хлора.
Зопиклон обладает свойством уменьшать время засыпания и частоту ночных и ранних пробуждений, увеличивать продолжительность сна и улучшать качество сна и пробуждения. Эти эффекты сочетаются с характерным ЭЭГ-профилем, который отличается от такового, регистрируемого при приеме бензодиазепинов. При бессоннице зопиклон сокращает I фазу, продлевает II фазу сна и сохраняет или продлевает стадии глубокого сна (III и V) и парадоксального (быстрого) сна. Сон наступает в течение 30 мин и продолжается 6–8 ч.
Применение зопиклона в течение 4 нед не вызывает значимой рикошетной бессонницы, а также ускользания снотворного эффекта (при приеме в течение до 17 нед).
Фармакокинетика
Абсорбция. После приема внутрь зопиклон быстро и полностью всасывается в ЖКТ. Cmax в плазме крови достигаются в пределах 1,5–2 ч и составляют приблизительно 30 и 60 нг/мл после приема внутрь 3,75 и 7,5 мг соответственно. Абсорбция зопиклона не зависит от пола, а также приема пищи.
Распределение. Связь с белками плазмы крови является слабой (составляет примерно 45%) и ненасыщаемой. Риск взаимодействия с другими препаратами на уровне связи с белком является очень низким. Зопиклон быстро распределяется из системного кровотока. Vd составляет 91,8–10,4 л. Зопиклон легко проходит через ГЭБ. Концентрации зопиклона в грудном молоке подобны таковым в плазме. Поступление зопиклона в организм ребенка вместе с грудным молоком не превышает 1% от дозы, принятой матерью в течение 24 ч.
Метаболизм. После повторных применений кумуляция зопиклона и его метаболитов не происходит. Межиндивидуальные отличия незначительные. Основными метаболитами являются производное N-оксида (фармакологически активный) и N-деметиловый метаболит (фармакологически неактивный). T1/2 составляет приблизительно 4,5 и 7,4 ч соответственно.
Выведение. В рекомендуемых дозах T1/2 неизмененного зопиклона составляет приблизительно 5 ч. Низкие значения почечного клиренса неизмененного зопиклона (8,4 мл/мин) по сравнению с его плазменным клиренсом (232 мл/мин) указывают на то, что клиренс зопиклона является преимущественно метаболическим. С мочой зопиклон выводится (приблизительно 80%) главным образом в виде метаболитов, с каловыми массами выводится приблизительно 16%.
Отдельные группы больных
Пожилой возраст.У пожилых больных, несмотря на небольшое снижение метаболизма в печени и удлинение T1/2 приблизительно до 7 ч, кумуляция зопиклона в плазме не была выявлена даже при многократном применении.
Почечная недостаточность. Кумуляция зопиклона или его метаболитов не была обнаружена даже после длительного приема.
Цирроз печени. В связи с уменьшением процесса деметилирования приблизительно на 40% уменьшается плазменный клиренс зопиклона, поэтому необходимо приспособление дозы.
Показания
Лечение преходящей, ситуационной и хронической бессонницы у взрослых (включая трудности с засыпанием, ночными и ранними пробуждениями).
Противопоказания
- гиперчувствительность к зопиклону или какой-либо составной части препарата;
- тяжелая дыхательная недостаточность;
- тяжелая псевдопаралитическая миастения (myasthenia gravis);
- тяжелая острая и хроническая печеночная недостаточность;
- синдром сонных апноэ;
- врожденная непереносимость галактозы, дефицит Lapp-лактазы, мальабсорбция глюкозы-галактозы;
- период кормления грудью;
- возраст до 18 лет.
С осторожностью: лица с алкогольной, наркотической или лекарственной зависимостью в анамнезе; пациенты, одновременно принимающие алкоголь или другие психотропные препараты (повышенный риск развития зависимости или злоупотребления).
Применение при беременности и кормлении грудью
Из-за отсутствия клинических данных и предосторожности в первых 3 мес беременности применение зопиклона не рекомендуется. Если все-таки необходимо применять зопиклон в последние 3 мес беременности, всегда по возможности следует применять минимальную эффективную дозу. Применение зопиклона в последнем триместре беременности может вызвать у новорожденного признаки гипотермии, гипотонию, угнетение дыхания и сонливость. В течение первых дней жизни может проявиться абстинентный синдром.
Если зопиклон назначается женщинам репродуктивного возраста, пациентки должны быть предупреждены о необходимости обратиться к врачу, чтобы принять решение о прекращении применения лекарства, если есть подозрение на беременность или она планируется.
Известно, что зопиклон выделяется в грудное молоко. Его применение кормящей матерью может вызвать седативный эффект у ребенка (слабость, сниженный тонус). Поэтому в период кормления грудью применение препарата Сомнол® следует прекратить.
Способ применения и дозы
Реклама: ООО «РЛС-Библиомед», ИНН 7714758963, erid=4CQwVszH9pUmKjt23pm
Внутрь. Препарат следует принимать непосредственно перед отходом к ночному сну.
Лечение должно быть по возможности кратковременным и не превышать 4 нед, включая период снижения дозы. Продление сроков лечения свыше максимально допустимых проводят после повторной оценки состояния больного. Лечение всегда следует начинать с наименьшей эффективной дозы и никогда не превышать максимальную дозу.
Рекомендуемые дозы
Взрослым пациентам моложе 65 лет — по 1 табл. 7,5 мг 1 раз в сутки.
Пациентам с нарушением функции почек лечение рекомендуется начинать с дозы, равной 3,75 мг (1/2 табл.) 1 раз в сутки, хотя кумуляция зопиклона или его метаболитов в случаях почечной недостаточности не отмечена.
Пациентам с нарушением функции печени лечение начинают с дозы 3,75 мг/сут, поскольку элиминация препарата у этой группы пациентов снижена. При необходимости дозу можно осторожно увеличивать до 7,5 мг/сут, принимая во внимание чувствительность пациента.
Пациентам с дыхательной недостаточностью назначают по 3,75 мг/сут.
Лечение пожилых пациентов старше 65 лет начинают с дозы 3,75 мг/сут. В случае необходимости дозу можно постепенно увеличивать, принимая во внимание индивидуальную чувствительность пациента.
Во всех случаях суточная доза не должна превышать 7,5 мг.
Длительность лечения
Преходящая бессонница — от 2 до 5 дней.
Ситуационная бессонница — от 2 до 3 нед.
Хроническая бессонница — длительность курсового лечения определяется после консультации со специалистом.
Побочные действия
Наиболее частый побочный эффект, наблюдаемый при назначении зопиклона, — горький или металлический вкус во рту. Также могут наблюдаться побочные эффекты, указанные ниже.
Расстройства пищеварения — диспепсия, тошнота, сухость во рту.
При пробуждении — сонливость, головокружение, головная боль, депрессия, агрессивность, антероградная амнезия, эйфория и нарушение координации движений.
Психические и парадоксальные реакции — ночные кошмары, замешательство, галлюцинации и поведенческие изменения, в т.ч. раздражительность, спутанность сознания, подавленное настроение, неадекватное поведение, которое возможно связано с амнезией, сомнамбулизм (снохождение), нарушение либидо. Эти побочные явления чаще наблюдаются у лиц пожилого возраста, но тяжелыми бывают редко.
Аллергические кожные реакции (зуд, высыпания), анафилактические реакции и/или ангионевротический отек.
Незначительное повышение в сыворотке крови активности трансаминаз и/или щелочной фосфатазы.
При прекращении терапии возможно возникновение рикошетной бессонницы (частое пробуждение, возобновление бессонницы или ее усиление) или появление лекарственной зависимости, но обычно это бывает после длительного применения. В очень редких случаях возможны судороги.
Взаимодействие
Не рекомендуется одновременный прием с алкоголем, т.к. алкоголь усиливает седативное действие препарата Сомнол®.
Усиление угнетающего влияния на ЦНС может встречаться в случаях одновременного назначения с антипсихотическими (нейролептическими) средствами, снотворными, транквилизаторами, седативными средствами, антидепрессантами, наркотическими анальгетиками, противосудорожными средствами, анестетиками, а также блокаторами H1-гистаминовых рецепторов, обладающими седативным эффектом. Перед совместным применением препарата Сомнол® с данными препаратами следует тщательно взвесить ожидаемый терапевтический эффект.
Препарат Сомнол® снижает концентрацию тримипрамина в плазме и его эффект.
Совместное применение препаратов, аналогичных производным бензодиазепина, и наркотических анальгетиков, включая опиаты и производные морфина (болеутоляющие средства, средства против кашля и терапия замены), может привести к усилению эйфории и повышению риска развития лекарственной зависимости.
Клозапин может увеличить риск шока с остановкой дыхания и/или сердца.
Совместное применение препарата Сомнол® с наркотическими анальгетиками и барбитуратами может вызвать риск угнетения дыхания. В случае передозировки возможен летальный исход.
Действие сходных с производными бензодиазепина ЛС усиливается, если они применяются в сочетании с ингибиторами печеночных ферментов, особенно цитохрома Р450 (в т.ч. антибиотик эритромицин, противогрибковые препараты итраконазол, кетоконазол).
Однако одновременное применение карбамазепина, фенитоина или рифампицина (усиливают активность печеночных ферментов) снижает терапевтический эффект препарата Сомнол®.
Передозировка
Симптомы: различной степени угнетения ЦНС — от сонливости до комы, в зависимости от количества принятого препарата. В легких случаях симптомы выражаются в сонливости, спутанности сознания, апатии. В более серьезных случаях симптомы могут выражаться в атаксии, летаргии, гипотонии, угнетении дыхания и коме. Редко — AV-блокада. Обычно это угнетение ЦНС не угрожает жизни пациента. Однако при совместном применении препарата Сомнол® с алкоголем или другими средствами, оказывающими угнетающее действие на ЦНС, передозировка может быть тяжелой и опасной для жизни пациента. Другие факторы риска, такие как сопутствующее заболевание и ослабленное состояние пациента, могут усиливать симптомы и даже (очень редко) привести к летальному исходу.
Лечение: назначение активированного угля, промывание желудка в течение 1 ч после передозировки. В случае выраженного угнетения ЦНС — флумазенил может быть использован как антидот (не использовать в случае сочетанной передозировки с другими ЛС и в качестве диагностического средства при передозировке неизвестных ЛС для постановки или исключения диагноза интоксикации бензодиазепинами). При необходимости рекомендуется симптоматическая и поддерживающая терапия в условиях стационара. Необходим контроль жизненно важных функций организма (дыхательная, сердечно-сосудистая). Гемодиализ имеет малую значимость из-за большого Vd зопиклона.
Особые указания
Оболочки таблеток препарата Сомнол® содержат краситель, в состав которого входит лактоза, поэтому пациентам с редкой врожденной непереносимостью галактозы, дефицитом Lapp-лактазы или мальабсорбцией глюкозы-галактозы нельзя назначать данное лекарство.
У пациентов с нарушением функции печени или почек, а также пожилых людей старше 65 лет и пациентов с дыхательной недостаточностью препарат Сомнол® применяют с осторожностью (рекомендуется снижение доз) (см. «Способ применения и дозы»).
Всегда при возможности следует выяснить причину бессонницы и перед назначением снотворного средства необходимо ликвидировать возможные вызывающие ее факторы.
Бензодиазепины и их аналоги не являются препаратами первого выбора при лечении психозов.
Риск развития зависимости
Во избежание возможного развития лекарственной зависимости курс лечения не должен превышать 4 нед.
Хотя риск минимален, нельзя абсолютно исключить развитие привыкания к препарату и злоупотребление им. Риск зависимости или злоупотребления возникает в случаях:
— превышения дозы и увеличения продолжительности лечения;
— злоупотребления алкоголем и/или другими ЛС;
— применения с алкоголем или другими психотропными препаратами;
— наличия тревожности.
При назначении препарата пациентам с наличием в анамнезе указаний на чрезмерное употребление алкоголя и/или зависимость от ЛС и пациентам с изменениями личности следует иметь в виду, что риск развития зависимости у них повышен. Эти пациенты должны находиться под тщательным контролем.
Синдром отмены и рикошетная бессонница
Риск таких явлений после резкого прекращения применения зопиклона не может быть исключен, особенно после длительного лечения. Поэтому рекомендуют постепенно уменьшать дозу и уведомлять об этом больного.
Если у пациента возникла физическая зависимость от данного препарата, внезапное прекращение его применения может привести к развитию синдрома отмены, для которого характерны следующие симптомы: бессонница, головная боль, мышечная боль, беспокойство, напряженность, возбуждение, нарушения сознания и раздражительность. В более тяжелых случаях могут наблюдаться следующие симптомы: нарушение восприятия реальности, деперсонализация, потеря чувствительности и онемение конечностей, повышенная чувствительность к шуму, свету и физическому контакту, галлюцинации и эпилептические судороги. Если длительность лечения не превышает 4 нед, возникновение симптомов отмены при прекращении применения лекарства маловероятно. Тем не менее, рекомендуется постепенное прекращение лечения. При прекращении приема препарата может развиться преходящий синдром рикошетной бессонницы с усиленным возобновлением симптомов, из-за которых было начато лечение; часто это тяжелая бессонница в сочетании с одним из упомянутых выше симптомов отмены. Данный синдром в основном проявляется при внезапном прекращении длительной терапии или при употреблении доз, превышающих рекомендованные дозы. Поэтому следует избегать внезапного прекращения приема препарата, его дозу следует снижать постепенно, проинформировав пациента о возможности возникновения и мерах предупреждения развития рикошетной бессонницы.
Амнезия
Может встречаться антероградная амнезия, если после приема таблетки вечером пациент все-таки просыпается ночью или не может уснуть или в случае, если отложен отход ко сну. Для снижения риска проявления антероградной амнезии необходимо:
— принимать таблетку непосредственно перед сном;
— обеспечить продолжительность сна не менее 7–8 ч.
Депрессия
Препарат не показан для лечения депрессии и может даже маскировать ее симптомы. Если бессонница связана с депрессией, то перед применением препарата Сомнол® ее нужно предотвратить. Препарат Сомнол® нельзя использовать в монотерапии для лечения депрессии и вызванной ею тревоги, поскольку они могут побудить к самоубийству.
Другие психические и парадоксальные реакции
У отдельных пациентов во время применения бензодиазепинов и их аналогов могут возникать парадоксальные реакции:
— усиление бессонницы и ночных кошмаров;
— нервозность, раздражительность, возбуждение, агрессивность и приступы гнева;
— делирий, галлюцинации, онирический делирий, психотические симптомы, неадекватное поведение и другие поведенческие расстройства.
Эти симптомы чаще всего могут проявляться у пожилых людей. Если это происходит, терапию следует прекратить.
Сомнамбулизм и связанное с ним поведение
У пациентов, которые принимали зопиклон и полностью не пробудились, отмечалось снохождение и другое аналогичное поведение, в т.ч. «вождение автомобиля», приготовление и прием пищи или разговор по телефону с последующей амнезией такого поведения. Употребление алкоголя и других средств, угнетающих ЦНС одновременно с зопиклоном повышает риск развития такого поведения, также как применение зопиклона в дозах, превышающих максимальные рекомендованные дозы. Прекращение терапии у пациентов, которые сообщают о таком поведении, должно быть строго взвешено.
Применение у детей
Эффективность и безопасность применения зопиклона у детей до 18 лет не установлены.
Влияние на способность управлять транспортными средствами и обслуживать движущиеся механизмы. Так как препарат Сомнол® относится к группе седативных средств, вызывающих сонливость, после приема препарата следует воздерживаться от управления транспортными средствами или выполнения работы оператора различных устройств и механизмов.
Форма выпуска
Таблетки, покрытые пленочной оболочкой, 7,5 мг. По 10 табл. в контурной ячейковой упаковке из алюминиевой фольги и пленки ПВХ с ПВДХ-покрытием. По 1 или 2 контурной ячейковой упаковки помещают в пачку из картона.
Производитель
АО «Гриндекс». Ул. Крустпилс, 53, Рига, LV-1057, Латвия.
Тел.: 371 67083205; факс: 371 67083505.
Электронная почта: grindeks@grindeks.lv
Организация, принимающая претензии: ООО «Гриндекс Рус». 117556, Москва, Варшавское ш., 74, корп. 3, эт. 5.
Тел.: (495) 771-65-05; факс: (499) 610-39-63.
Электронная почта: office@grindeks.ru
Условия отпуска из аптек
По рецепту.
Условия хранения
В защищенном от света месте, при температуре не выше 25 °C.
Хранить в недоступном для детей месте.
Срок годности
3 года.
Не применять по истечении срока годности, указанного на упаковке.
Представленная информация о ценах на препараты не является предложением о продаже или покупке товара.
Информация предназначена исключительно для сравнения цен в стационарных аптеках, осуществляющих деятельность в
соответствии со статьей 55 Федерального закона «Об обращении лекарственных средств» от 12.04.2010 № 61-ФЗ.